About onethird of men over 50 have low bone mass, and roughly6% already meet the clinical definition of osteoporosis. The risk climbs sharply after 70years. Below youll find the latest numbers, why men get it, how to spot the signs, and what you can actually do to stay strongboned all explained in plain, friendly language.
Current Landscape
What do the latest statistics say?
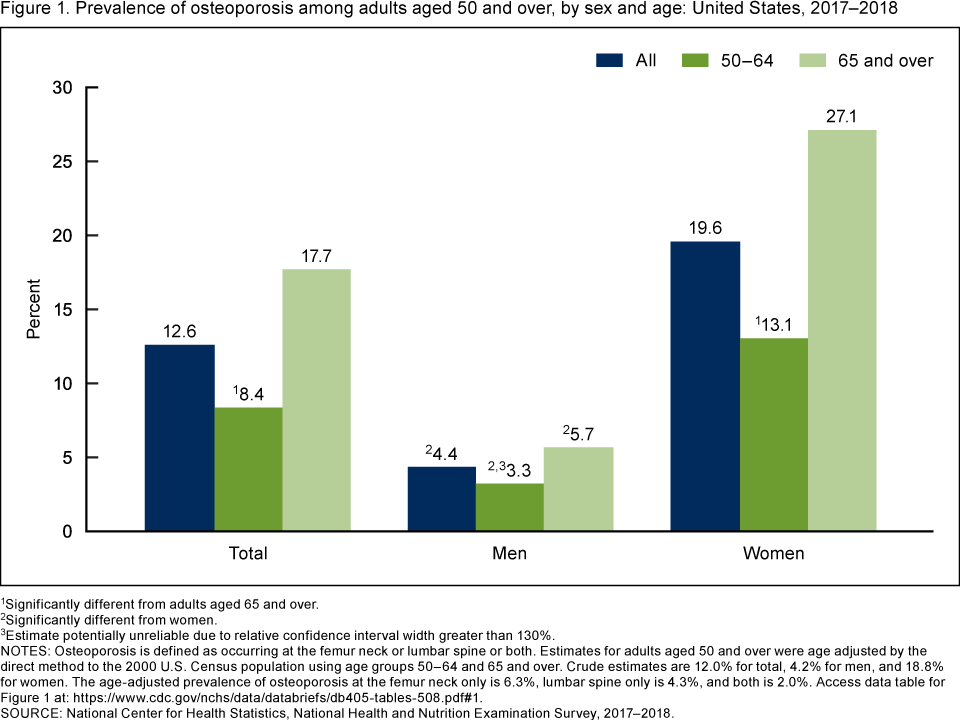
Recent data from the U.S. Centers for Disease Control and Prevention (CDC) show that 33.5% of men aged50and older have low bone mass, while 6.6% meet the osteoporosis threshold. In Europe, a 2023 study found the prevalence jumps to 16.6% in men over80years. Compared with womenwho hover around51% for low bone massmen still face a substantial burden, just often hidden in the background.
How has prevalence changed over the past decade?
Between 2007 and 2018 the U.S. saw a plateau in male osteoporosis rates, while womens rates rose modestly. The flat trend for men may stem from underdiagnosis: doctors are less likely to order a DEXA scan for a man unless a fracture occurs, so many cases slip through the cracks.
Why is male osteoporosis often underestimated?
Research published in points out two big factors: first, media and public health campaigns focus heavily on women, so men assume theyre safe; second, clinicians sometimes view bone loss as a womens disease, leading to fewer screenings.
Whos at Risk
Primary (nonmodifiable) risk factors
- Age50years bone turnover speeds up and calcium absorption drops.
- Family history a parent or sibling with osteoporosis raises your odds.
- Ethnicity Caucasian and Asian men are more prone than AfricanAmerican men.
Secondary (modifiable) risk factors
- Hormonal changes: low testosterone or hyperparathyroidism can fasttrack bone loss.
- Medical conditions: chronic obstructive pulmonary disease, rheumatoid arthritis, inflammatory bowel disease, and kidney disease all interfere with bone health.
- Medications: longterm glucocorticoids, anticonvulsants, and even protonpump inhibitors can gnaw away at bone density.
Lifestyle contributors
- Smoking it reduces blood flow to boneforming cells.
- Excess alcohol more than two drinks a day impairs calcium balance.
- Sedentary life weightbearing activity is the natural exercise for your skeleton.
- Low calcium or vitaminD intake you cant build bone without the raw materials.
What causes osteoporosis in young males?
Its rare, but when it happens its usually tied to genetics or endocrine quirks. Conditions like osteogenesis imperfecta, hypophosphatasia, or Klinefelter syndrome can strip bone strength in the 20s and 30s. Even prolonged steroid use for asthma or autoimmune disease can act as a fastforward button on bone loss.
Realworld example
Meet Alex, a 38yearold marathon runner who felt a sharp twinge in his lower back after a slow jog. An Xray revealed a tiny vertebral fracture. A DEXA scan showed a Tscore of2.6, confirming osteoporosis. His story underscores that young, fit doesnt guarantee immunity especially when hidden hormonal imbalances are at play.
Spotting Symptoms
Common (and often missed) signs
- Persistent, dull back pain often the first hint of a vertebral compression fracture.
- Loss of height or a stooped posture the shrinking effect of collapsed vertebrae.
- Frequent fractures from minor falls a broken wrist from tripping on a carpet could be a red flag.
How doctors assess bone health
The gold standard is a DEXA (dualenergy Xray absorptiometry) scan. A Tscore2.5 confirms osteoporosis. For detailed trabecular analysis, some specialists use peripheral quantitative CT (pQCT), though its less common.
Male bone density chart interpreting results
Below is a simplified male bone density chart by age. Your doctor will compare your score to these reference ranges.
| Age Range | Typical TScore | Interpretation |
|---|---|---|
| 3039 | 0.5 to0 | Normal, high peak bone mass |
| 4049 | 0.8 to0.2 | Low bone mass possible |
| 5059 | 1.0 to0.5 | Low bone mass (osteopenia) |
| 6069 | 1.5 to0.8 | Increasing risk |
| 70 | 2.0 or lower | High risk for osteoporosis |
Men vs Women a quick comparison
| Metric | Men50yr | Women50yr |
|---|---|---|
| Low bone mass prevalence | 33.5% | 51.5% |
| Osteoporosis prevalence | 6% | 1520% |
| Hipfracture incidence (per 1,000) | 4.5 | 12.0 |
Even though women have higher rates, men often present later and with more severe fractures because theyre not screened as early. Thats why awareness matters for both genders.
Men vs Women
Epidemiology sidebyside
Men experience roughly onethird of all fragility fractures, yet they account for about 40% of fracturerelated deaths. The gap is partly due to later diagnosis and a higher prevalence of comorbidities like heart disease that complicate recovery.
Biological reasons for disparity
Men typically achieve a higher peak bone mass during their 20s. Testosterone also stimulates osteoblast activity (the cells that build bone). When testosterone declines with age, bone loss accelerates, mirroring the estrogen drop women experience after menopause.
Clinical implications
Because men often ignore early warning signs, they may suffer a hip fracture that could have been prevented with earlier intervention. Encouraging routine bone health checks at age50regardless of genderhelps close that gap.
Treatment Options
Firstline pharmacotherapy
Bisphosphonates (alendronate, risedronate) remain the goto oral drugs. They bind to bone and slow the cells that break it down. For men who struggle with daily pills, an annual IV infusion of zoledronate offers a convenient alternative.
Hormonal & targeted therapies
- Testosterone replacement appropriate for men with documented low levels, it can modestly improve bone density.
- Denosumab a monthly injection that blocks a protein called RANKL, reducing bone resorption.
- Romosozumab a newer boneforming antibody, typically reserved for highrisk patients.
Treatment of osteoporosis in elderly males
Older men often have reduced kidney function, so doctors must choose medications carefully. Oral bisphosphonates can cause esophageal irritation, while IV options require monitoring of calcium levels. A thorough medication review is essential before starting therapy.
Lifestyle & supplemental support
- Calcium intake of at least 1,200mg daily (milk, leafy greens, fortified foods).
- VitaminD8001,000IU daily sunshine or a supplement helps calcium absorption.
- Weightbearing and resistance training think squats, kettlebell swings, or brisk walking with a backpack.
- Quit smoking and limit alcohol even small changes can tilt the balance in favor of bone health.
Monitoring & followup
Repeating a DEXA scan every 23years lets you track progress. In the meantime, use the FRAX calculator (with malespecific inputs) to gauge your 10year fracture risk and adjust treatment accordingly.
Success story
John, a 65yearold retiree, started alendronate and a calciumvitaminD regimen after a wrist fracture. Two years later his FRAX score dropped from 22% to 8%, and a repeat DEXA showed a 4% increase in lumbar spine density. His experience illustrates that timely treatment really does pay off.
Prevention Habits
Prevention isnt about a single miracle; its a collection of daily choices that together keep your skeleton sturdy.
| Prevention Pillar | Action Items | Why It Helps |
|---|---|---|
| Nutrition | Consume dairy, fortified plant milks, leafy greens; aim for 1,200mg calcium & 1,000IU vitaminD. | Provides the minerals bones need to rebuild. |
| Physical Activity | 30minutes of moderate weightbearing exercise 5/week (e.g., walking, jogging, resistance training). | Stimulates osteoblasts to produce new bone. |
| Lifestyle | Quit smoking, limit alcohol to 2 drinks/day. | Reduces boneresorbing chemicals in the bloodstream. |
| Medical Screening | Baseline DEXA at 50yr (earlier if you have risk factors). | Early detection lets you intervene before fractures. |
Downloadable checklists are a great way to keep yourself accountable you can print one and tick off each habit as you go.
Expert Sources
Suggested credible citations
- CDC Data BriefDB405 (2022) national prevalence figures.
- Osteoporosis in Men: A Review of an Underestimated Bone Condition Journal of Bone and Mineral Research (2021).
- comprehensive epidemiologic analysis.
- American Academy of Family Physicians practice guidelines (2003) screening recommendations.
Expert commentary ideas
Consider adding a short quote from an endocrinologist about testosterones role, or a geriatricians take on managing bone health in frail seniors. These voices boost authoritativeness and reassure readers that the advice is medically sound.
Conclusion
Men over 50 face a real, often hidden risk of osteoporosisabout33% have low bone mass and6% meet the diagnostic threshold. Age, hormones, lifestyle, and certain illnesses are the main drivers, while early signs are subtle and easy to miss. The good news? A reliable DEXA scan, evidencebased medications, and simple daily habits (calcium, vitaminD, weightbearing exercise, quitting smoking) can dramatically cut your fracture risk. If youre approaching 50 or have any of the risk factors mentioned, schedule a bonedensity test and start a conversation with your doctor. Stay proactive, stay informed, and keep those bones strong for the adventures that lie ahead.
FAQs
At what age should men begin osteoporosis screening?
Most guidelines recommend a baseline DEXA scan at age 50 for men, or earlier if they have risk factors such as a family history of fractures, chronic steroid use, or low testosterone.
How does testosterone influence bone health in men?
Testosterone stimulates osteoblast activity, the cells that build bone. A decline in testosterone with age speeds up bone loss, making men more susceptible to osteoporosis.
Which foods provide the best nutrients for strengthening male bones?
Calcium‑rich options like dairy, fortified plant milks, leafy greens, and sardines, combined with vitamin D sources (fatty fish, eggs, sunlight exposure or supplements), support bone formation and mineralization.
Can regular exercise actually reverse low bone mass in men over 50?
Weight‑bearing and resistance training (e.g., walking, jogging, squats, kettlebell swings) can increase bone density modestly and improve balance, reducing fracture risk even after bone loss has begun.
What are the most common medications prescribed for male osteoporosis?
First‑line treatments include oral bisphosphonates (alendronate, risedronate) and the yearly IV infusion zoledronate. For men with specific needs, denosumab injections, testosterone replacement (when deficient), or the newer bone‑forming agent romosozumab may be used.