At first I thought the night sweats and the sudden stiffness in my lower back were just typical menopause symptoms. Then the pain lingered longer than a hot flash, and I realized my
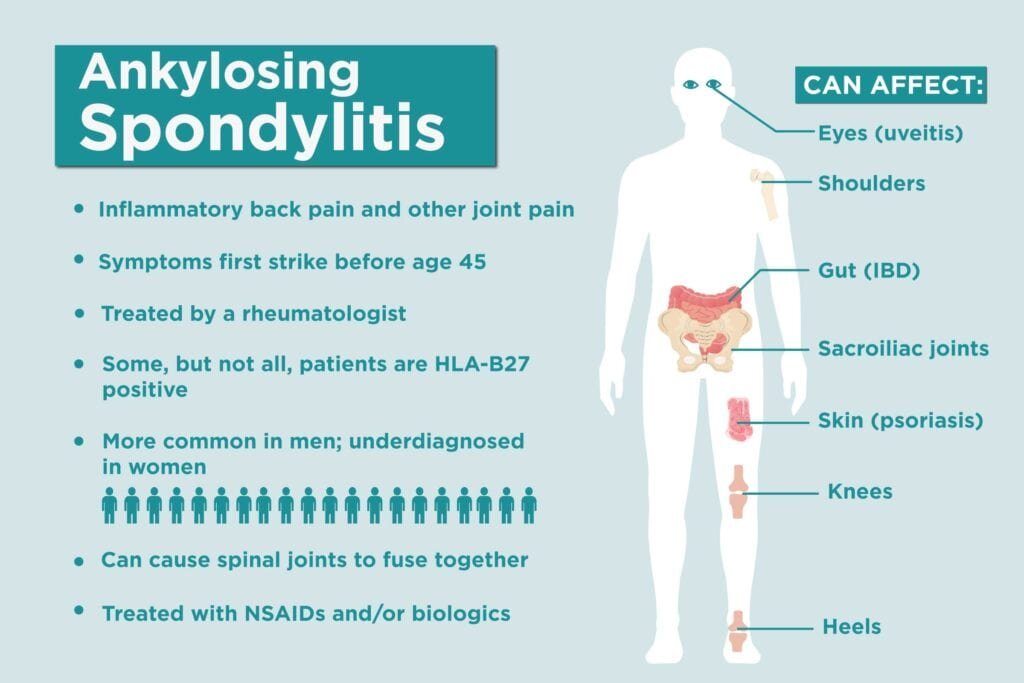
ankylosing spondylitis (AS) was quietly turning up the volume. If you're a woman navigating both menopause and AS, you're probably wondering whether the two are connected and what you can actually do about it.Bottom line: menopause can amplify AS discomfort, shift how hormones interact with inflammation, and mess with your bone health balancebut with the right knowledge, medication tweaks, and everyday habits, you can keep flare-ups under control and enjoy this new chapter.## Why Menopause Matters### Hormonal shifts that matterMenopause signals a steep decline in estrogen and progesterone. Those hormones do more than regulate your cycle; they play a protective role for bones and modulate inflammatory pathways. When estrogen drops, the body's natural brake on inflammation loosens, which can make the chronic inflammation of ankylosing spondylitis feel louder.### Inflammation meets ASResearch explains that estrogen interacts with cytokinesthose messenger molecules that drive inflammation. Less estrogen means cytokines like TNF and IL17 can become more active, potentially worsening spinal pain and stiffness.### Vitamin D's hidden roleLow estrogen also reduces the skin's ability to synthesize vitamin D, which is crucial for bone remodeling. A 2023 PubMed review highlighted that postmenopausal women with AS often present lower vitamin D levels, linking the deficiency to both increased pain and higher fracture risk.## Common Female Symptoms### Back pain that won't quitMany women report that the classic morning stiffness of AS turns into a persistent ache that lingers through the day, especially after a night of hot flashes. The combination of hormonal turbulence and
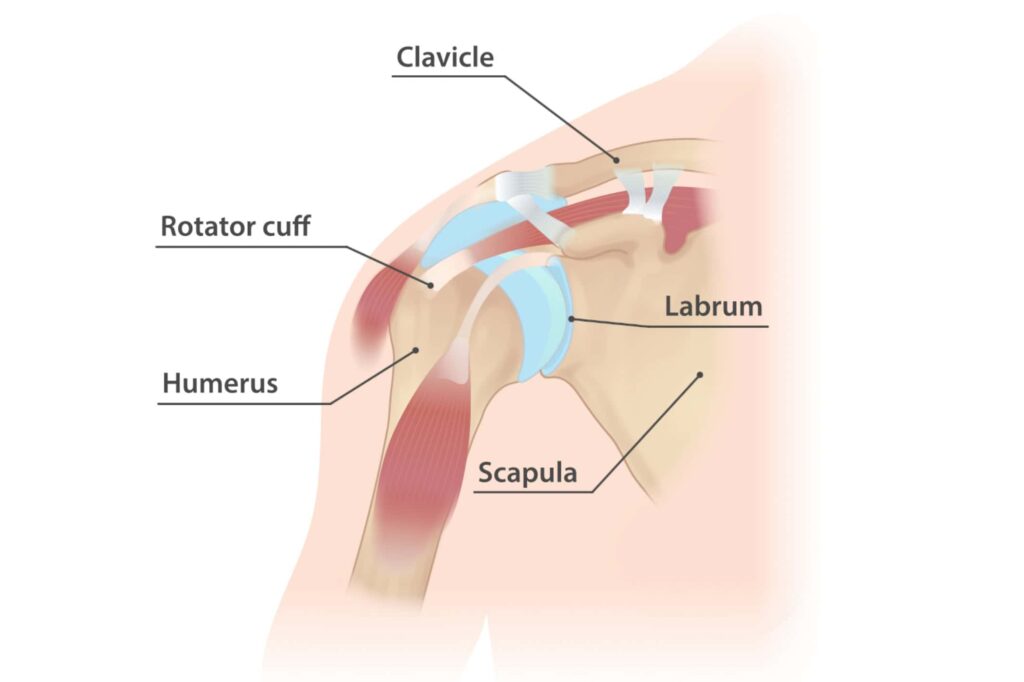
spine inflammation can make each movement feel like you're pulling a rubber band.### Bloating and gut woesAnkylosing spondylitis bloated stomach isn't a typoit's a genuine complaint. Hormonal changes influence gut motility, and AS already predisposes many to IBS-type symptoms. If you notice a swollen belly that doesn't disappear after a light walk, it could be a double hit from both menopause and AS.### Joint pain beyond the spineWomen often feel pain in the hips, knees, and even the shouldersareas that men with AS might not emphasize as much. A recent Everyday Health article noted that up to 40% of female AS patients experience extra-axial joint discomfort during menopause.### Fatigue, mood swings, and sleep disruptionThese are classic menopause signs, but they're amplified when chronic pain keeps you up at night. The overlap can feel like a perfect storm, making it hard to separate just hormonal from AS-related.## Hormone Replacement Therapy### Can estrogen ease joint pain?Some studies suggest that low-dose estrogen therapy can modestly reduce musculoskeletal pain in postmenopausal women. According to , patients who added HRT to their regimen reported fewer flare-ups, though results varied.### Potential downsidesHRT isn't a free pass. Risks include blood clots, certain cancers, and possible interactions with biologic medications. The safest approach is a personalized risk-benefit analysis with your rheumatologist.
| HRT Type | Pros for AS | Cons / Risks |
|---|
| Oral estrogen | Easy dosing, proven systemic effect | Higher clot risk, liver metabolism |
| Transdermal patch | Lower clot risk, steady hormone levels | Skin irritation possible |
| Combined estrogen-progesterone | Balances uterine protection | Increased breast tenderness, possible mood changes |
### Talking to your doctorStart the conversation with something like, "I've noticed my AS pain spikes during menopause. Could HRT be part of a balanced plan?" Bring a list of your current medsespecially any TNF inhibitors or IL17 blockersso your doctor can spot interactions before they happen.## Managing Pain Safely### Medication tweaksNSAIDs remain a first-line option, but many women with AS also need biologics (e.g., adalimumab, secukinumab). When HRT is on board, choose biologics with minimal hepatic metabolism to avoid overloading the liver. A quick pros/cons chart can help you visualize the safest combo.### Physical therapy and targeted exercisesGentle mobility work is a lifesaver. Focus on lumbar flexion, hip opening, and thoracic rotation. Here's a 10-minute daily stretch you can do while your coffee brews:
- Cat-Cow (1-minute)
- Supine knee-to-chest (30 seconds each side)
- Seated spinal twist (30 seconds each side)
- Hip flexor stretch on a block (1-minute each side)
- Standing forward fold, letting gravity do the work (1-minute)
### Complementary approachesOmega-3 fish oil, magnesium, and yoga have modest evidence for reducing inflammation. A small randomized trial published in 2022 found that 2g of fish oil daily lowered ESR (a blood inflammation marker) in AS patients. If you're curious, try a six-week fish-oil-plus-stretch challenge and track your pain scores.### Personal story: How I cured my ankylosing spondylitisThat headline sounds like clickbait, but for me it meant a six-month commitment to a low-inflammatory diet, consistent physiotherapy, and a carefully chosen biologic. I didn't cure the diseaseAS is chronicbut I
achieved remission, meaning I could finally enjoy a hot yoga class without fearing a flare-up the next day.## Reproductive Health Overlap### Pregnancy after menopause?While natural conception isn't an option postmenopause, assisted reproductive technologies (ART) with hormone support can help some women. The AxSpA support program notes that women on biologics should switch to a pregnancy-compatible medication (like certolizumab) several months before embryo transfer.### Endometriosis and ASResearch on a direct link is scarce, but both conditions involve chronic inflammation. Some clinicians observe that women with severe endometriosis report heightened spinal pain, suggesting a possible overlap in inflammatory pathways.### Hysterectomy's impactRemoving the uterus often triggers a sudden drop in estrogen, similar to menopause. A case study described a patient whose AS pain temporarily intensified after hysterectomy, only to stabilize after HRT initiation. It underscores the importance of hormone monitoring after major gynecologic surgery.## Lifestyle Hacks### Bone health strategyAim for 1,200mg of calcium and 8001,000IU of vitamin D daily. Dairy, fortified plant milks, and leafy greens are excellent sources. If you struggle with absorption, a vitamin D3 supplement (2,000IU) is a safe starterjust check with your doctor.### Stress management & sleep hygieneStress spikes cytokine production, so calming the nervous system is essential. Try a 5-minute breathing exercise before bed: inhale for four counts, hold for four, exhale for six. Pair this with a cool-room environment (around 18C) to reduce night sweats and improve sleep quality.### Anti-inflammatory dietA Mediterranean-style platethink olive oil, fatty fish, nuts, and colorful veggieshas the best evidence for lowering systemic inflammation. Here's a quick grocery list:
- Salmon or mackerel (twice a week)
- Extra-virgin olive oil (use for cooking)
- Walnuts and almonds
- Spinach, kale, bell peppers
- Turmeric spice (add to soups)
### Daily movement mantraEven a brisk 15-minute walk can keep joints lubricated and mood lifted. When you're feeling a hot flash, swing your arms, do a light jog in place, or simply stretchmovement often blunts the intensity of both heat and pain.## Trusted Resources### Specialist directoriesLook for rheumatologists who list women's health or menopause as a focus area. Many hospitals now have multidisciplinary clinics that pair rheumatology with endocrinologyperfect for navigating the hormone-inflammation crossroads.### Support groups & podcastsOne of my favorite resources is the Navigating Menopause with Spondyloarthritis podcast, where clinicians and patients share real-world tips. Hearing someone say, "I felt the same way during my first hot flash," can feel like a hug on a tough day.### Online referencesReliable articles from , the AxSpA Australia education portal, and up-to-date PubMed reviews provide the scientific backbone for any decisions you make.## ConclusionMenopause doesn't have to be a villain in your ankylosing spondylitis story. By understanding how hormone shifts can amplify inflammation, exploring safe HRT options, adjusting medications, and embracing supportive lifestyle habits, you can keep flare-ups in check and feel more in control of your body. Remember, you're not alonelean on trusted specialists, join supportive communities, and never hesitate to ask your doctor the tough questions. If this guide resonated with you, share your experiences in the comments or grab our free symptom-tracker sheet so we can all navigate this journey together.
FAQs
How does menopause affect ankylosing spondylitis symptoms?
During menopause estrogen and progesterone levels drop, removing a natural brake on inflammation. This can make the chronic inflammation of AS feel louder, leading to increased spinal pain, stiffness, and flare‑ups.
Can hormone replacement therapy help reduce AS pain?
Low‑dose estrogen therapy has been shown in some studies to modestly lessen musculoskeletal pain in post‑menopausal women. However, HRT carries risks (blood clots, certain cancers) and may interact with biologic meds, so a personalized risk‑benefit discussion with your rheumatologist is essential.
What safe medications can I use for AS during menopause?
NSAIDs remain first‑line, but many women also need biologics (adalimumab, secukinumab, etc.). When HRT is added, choose biologics with minimal liver metabolism and monitor for interactions. Always review your full medication list with your doctor.
Which exercises are best for managing spinal stiffness in menopause?
Gentle, daily mobility work helps keep the spine supple. Focus on lumbar flexion, hip opening, and thoracic rotation. A quick 10‑minute routine (cat‑cow, knee‑to‑chest, seated twist, hip flexor stretch, standing forward fold) can be done while your coffee brews.
How can I protect my bones while dealing with AS and menopause?
Aim for 1,200 mg calcium and 800‑1,000 IU vitamin D daily through diet and supplements. Include weight‑bearing activities, ensure adequate protein, and consider a vitamin D3 supplement (2,000 IU) if levels are low. Regular bone‑density scans are advised.