Ever feel like your shoulder moves a bit too freely, or that a simple stretch suddenly turns into a painful snap? Thats a hypermobile shoulderyour joint's range of motion exceeds the usual limits because the surrounding ligaments and capsule are a little too lax. It can be a hidden source of shoulder pain, instability, or just that weird double-jointed feeling. Below you'll find exactly what it is, how to spot it, and what you can do to stay strong, comfy, and pain-free.
What Is Hypermobile Shoulder?
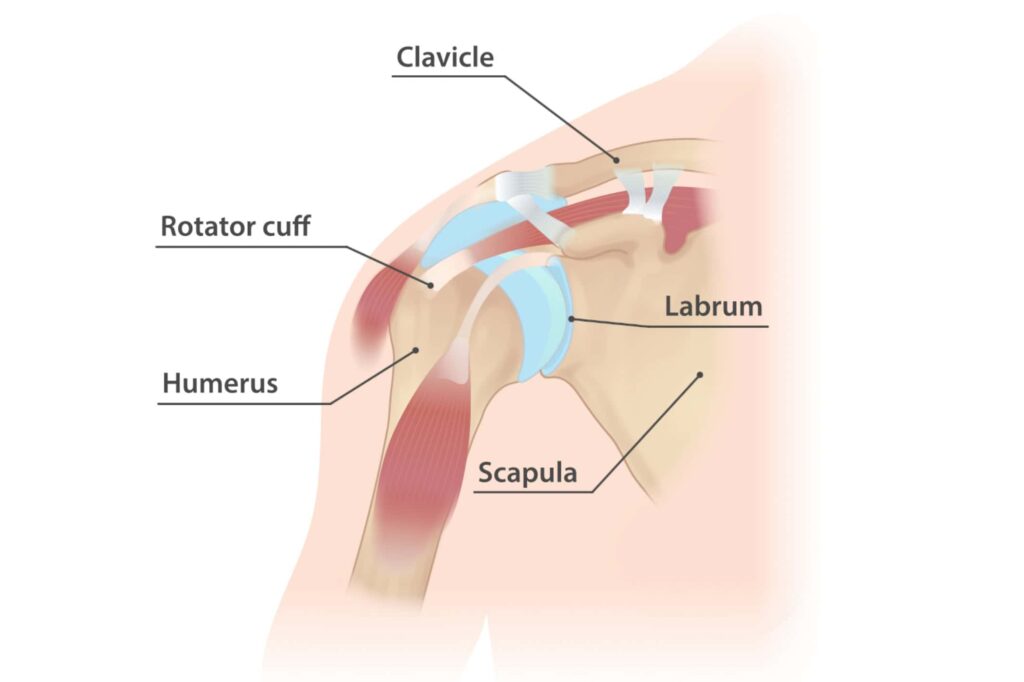
Definition & Anatomy
In a typical shoulder, strong ligaments and a tight joint capsule keep the ball-and-socket joint nicely centered. When those structures are looser, the humeral head can glide farther than normalthis is what we call a hypermobile shoulder. Think of it as a door hinge that's been over-lubricated; it swings wider but can wobble if you don't watch it.
Common Causes
- Genetic factors (e.g., Ehlers-Danlos syndrome or other collagen disorders)
- Repeated overhead activities (yoga, swimming, weightlifting)
- Previous injuries that stretched the capsule
- Natural variationsome people are just born with more flexible joints
Who's at Risk?
Anyone can have a hypermobile shoulder, but you'll see it more often in:
- Athletes who demand extreme range of motion (gymnasts, swimmers, rock climbers)
- People with a family history of joint hypermobility
- Young adults, especially women, who are naturally more supple
Benefits & Risks
Extra mobility can be a superpower in activities that require fluid movement, yet it also brings a higher chance of instability, impingement, and chronic shoulder pain. Balancing the upside with the downside is the key to thriving with a hypermobile shoulder.
| Aspect | Hypermobile Shoulder | Normal Shoulder |
|---|---|---|
| Range of Motion | Exceeds typical limits (often >30 extra flexion/extension) | Standard anatomical limits |
| Stability | Reduced passive stability; relies more on muscle control | Balanced passive and active stability |
| Common Symptoms | Feeling of looseness, occasional popping, occasional pain | Rarely feels loose or double-jointed |
How to Identify It
Self-Assessment Checklist
Grab a pen and tick any that sound familiar:
- Can you raise your arm overhead more than most people?
- Do you often hear clicking or popping in the shoulder?
- Does your shoulder feel loose after a night of sleep?
- Have you experienced occasional subluxations (partial dislocations) without a clear injury?
If you answered yes to several, you might have a hypermobile shoulder.
Clinical Shoulder Hypermobility Test
The gold-standard test used by physiotherapists is the Glenohumeral Translation Test. The clinician grasps the top of your humeral head and gently pushes it forward, backward, and side-to-side. Excessive movement (more than 2cm) suggests hypermobility. Many clinics also incorporate the a quick 9-point system that includes shoulder flexibility as one of its items.
When to See a Professional
If you notice any of the following, schedule an appointment:
- Sharp or persistent shoulder pain, especially at night
- Recurrent dislocations or subluxations
- Swelling or a feeling of giving way during everyday tasks
- Loss of strength that interferes with work or sport
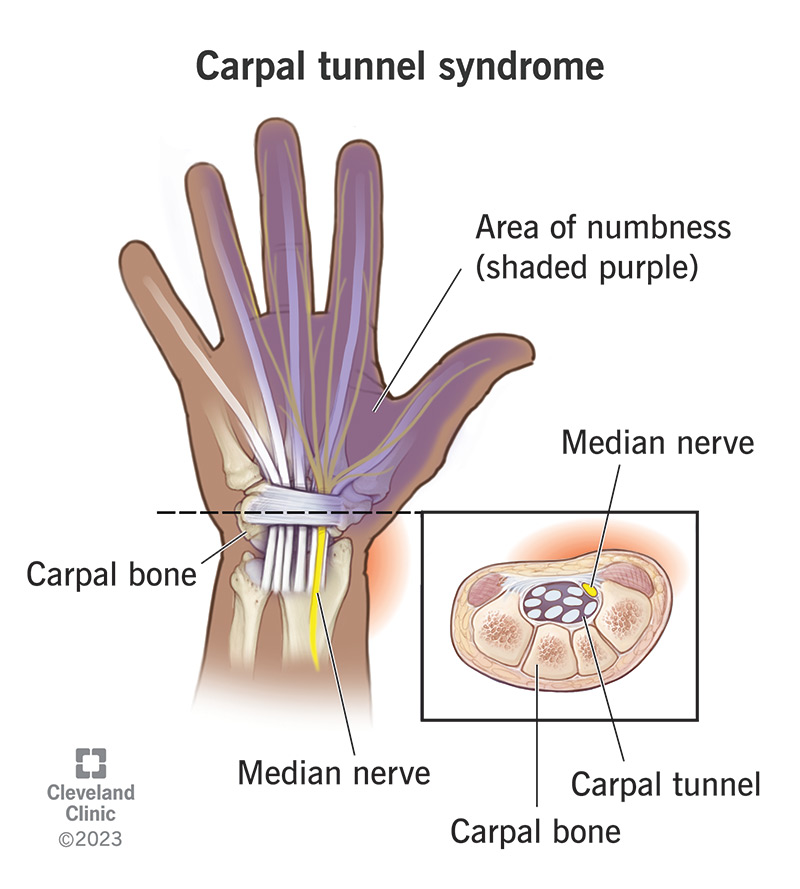
For persistent or unexplained hand swelling that accompanies shoulder symptoms, it's especially important to seek medical advice, as this could indicate more complex joint or systemic issues.
Differential Diagnosis
It's easy to mistake a hypermobile shoulder for other problems. Here's how it differs from a few common shoulder issues:
| Condition | Main Symptoms | Key Distinguishing Feature |
|---|---|---|
| Rotator-Cuff Tear | Deep ache, weakness when lifting | Pain worsens with resisted external rotation; not primarily loose |
| Impingement Syndrome | Sharp pain when raising arm above 90 | Compression of tendons; limited rather than excessive motion |
| True Instability | Frequent dislocations, feeling of falling out | Often follows trauma; hypermobility contributes but isn't the sole cause |
Managing Your Hypermobile Shoulder
Conservative (Non-Surgical) Treatment
Most people thrive with a structured physiotherapy program that emphasizes scapular control and rotator-cuff strength. A good therapist will teach you how to tighten the chassis of your shoulder, so the muscles compensate for the lax ligaments.
Targeted Hypermobile Shoulder Exercises
Below is a starter routine you can do 34 times a week. All movements should be pain-free; stop if you feel any sharp ache.
- Scapular Retraction (Band Pull-Apart) 3 sets of 12 reps. Keeps the shoulder blades glued to the back wall.
- Closed-Chain Row (Bodyweight on a table) 310. Encourages joint stability while moving in a safe plane.
- Isometric External Rotation Hold 10 seconds, 5 reps each side. Builds rotator-cuff endurance without excessive stretch.
- Wall Angel 215 slow slides. Improves posture and mobilizes the thoracic spine, which indirectly supports shoulder stability.
Over time, you can progress to light dumbbells, but always keep the movement controlled.
Pain Management
When soreness spikes, try alternating ice (15 min) and gentle heat (10 min) to calm inflammation and improve blood flow. Over-the-counter NSAIDs can help for a few days, but they're a band-aidnot a fix.
If you have other joint or bone concernslike osteoporosis physical therapy or osteoporosis rehablet your healthcare provider know, as this can influence your exercise plan and overall management.
Sleeping Hacks for a Hypermobile Shoulder
Getting a good night's rest is harder when your shoulder feels like it could pop out at any moment. Here's what works for many:
- Place a firm pillow under the affected arm to keep it slightly elevated and prevent it from rolling forward.
- Use a body pillow or a rolled-up towel behind your back to stop you from turning onto the painful side.
- Choose a mattress that offers medium supporttoo soft will let the shoulder sink, too hard will increase pressure points.
When Surgery Becomes Necessary
Only a minority of hypermobile shoulder sufferers need an operation. Surgical options include capsular plication (tightening the capsule) or labral repair if there's a tear. Success rates are high when the procedure is paired with a post-op rehab plan. Most patients regain functional stability within 612 months after surgery.
Long-Term Maintenance
Think of your shoulder like a car: regular tune-ups (strength sessions), oil changes (flexibility work), and check-ups (periodic professional assessments) keep it running smoothly. Set a reminder to reassess your range of motion and strength every three months.
Real World Stories
Case Study 1: Yoga Instructor
Emma, 28, teaches Vinyasa classes and noticed she could easily do reverse plank poses that left her students scrambling. However, after several weeks she started feeling a dull ache after long sessions. A physiotherapist performed the Glenohumeral Translation Test and confirmed hypermobility. Emma followed a 4-week scapular-strengthening program, added targeted rotator-cuff work, and within a month reported no more nagging soreness and even improved her arm balances. "I finally felt in control of my joints," she told me.
Case Study 2: Competitive Swimmer
Javier, 21, swam for his university team. He could glide through the water with astonishing ease, but occasional clicks turned into full-blown subluxations during high-intensity sets. After consulting a sports doctor, he began a rehab protocol focusing on closed-chain rowing and scapular stabilization. Six weeks later, his subluxations dropped from three per week to zero, and his personal best in the 100m freestyle improved by 0.3 seconds. "It wasn't about limiting my strokes; it was about making my shoulders smarter," he said.
Reddit Voices
On the r/Hypermobility subreddit, members frequently share practical tipslike using a shoulder strap during pull-ups or rotating through dynamic warm-up circuits before yoga. One user summed it up: "Know your limits, train your stabilizers, and never ignore that little acheit's a signal, not a verdict."
Top Helpful Resources
- Peer-Reviewed Study on Shoulder Instability in Ehlers-Danlos
Conclusion
Living with a hypermobile shoulder doesn't have to be a constant battle of pain and uncertainty. By understanding the anatomy, recognizing the signs, and committing to a balanced program of strength, stability, and smart lifestyle tweaks (like better sleep positioning), you can keep your joints happy and your life active. Remember, every shoulder is uniquelisten to its signals, seek professional guidance when needed, and stay consistent with the exercises that give you control.
What's your story? Have you discovered a trick that helped you manage shoulder hypermobility? Share your experiences in the comments below, and let's keep the conversation going. If you have any lingering questions, feel free to askI'm here to help you navigate the path to a stronger, more reliable shoulder.
FAQs
How can I tell if my shoulder is hypermobile?
You can start with a simple self‑assessment: notice if you can raise your arm higher than most, hear frequent clicks, or feel a “loose” sensation after sleep. Clinicians confirm hypermobility with the Glenohumeral Translation Test and may use the Beighton Score.
What exercises are safest for a hypermobile shoulder?
Focus on strengthening the stabilizers without excessive stretch. Good starter moves are scapular retraction band pull‑aparts, closed‑chain rows, isometric external rotation holds, and wall angels. Perform them pain‑free 3‑4 times a week and progress gradually.
Can hypermobility lead to long‑term shoulder problems?
Yes. Persistent laxity can increase the risk of instability, impingement, rotator‑cuff strain, and early arthritic changes. Regular strengthening and posture work help protect the joint and prevent chronic issues.
Is surgery ever needed for a hypermobile shoulder?
Surgery is rare and only considered when conservative care fails and there’s significant instability or labral damage. Options include capsular plication to tighten the capsule or arthroscopic labral repair, followed by a structured rehab program.
What sleeping positions help reduce shoulder discomfort?
Place a firm pillow under the affected arm to keep it slightly elevated, use a body pillow or rolled towel behind your back to avoid rolling onto the painful side, and choose a medium‑firm mattress that supports without sinking.