What is Rett
In a nutshell, Rett syndrome is caused by mutations in the MECP2 gene, which sits on the X chromosome. This gene is like a master switch for brain development; when its altered, the brains wiring goes awry after a period of apparently normal growth. The result is a cascade of regression in skills that were once mastered.
Genetics behind the scenes
The condition follows an Xlinked dominant pattern. Because girls have two X chromosomes, a single faulty copy can be buffered by the healthy one, which is why most patients are female. Boys, on the other hand, usually face a much more severe form or dont survive past infancy. in plain language.
How common is it?
Rett syndrome affects roughly 1 in 9,00010,000 live female births worldwide. The numbers vary a bit by region, but the rarity underscores the importance of accurate information when you finally encounter it.
| Region | Estimated prevalence (per 10,000 females) |
|---|---|
| North America | 1.01.2 |
| Europe | 0.91.1 |
| Asia | 0.70.9 |
Why mainly females
Ever wonder why you rarely hear about boys with Rett? Its all about the X chromosome. Girls carry two copies, so if one is mutated, the other can sometimes compensate, allowing survival but with the classic syndrome. Boys have only one X; a mutation there often leads to more severe outcomes, sometimes resulting in early miscarriage or a completely different clinical picture.
Male cases
When boys do have a MECP2 mutation, its usually a mosaic pattern (some cells have the mutation, others dont) or part of a broader chromosomal anomaly. These cases are rare, and the symptoms often diverge from the classic handwringing picture we associate with girls. provides a thorough overview of those atypical presentations.
Early signs
Most girls with Rett appear perfectly typical for the first six months of life. Then, somewhere between 6 and 18 months, the regression startsoften without warning.
Core regression symptoms
- Loss of purposeful hand skills (the infamous handwringing or clapping)
- Decline in spoken language, sometimes to the point of being nonverbal
- Gait abnormalities: a stiff, shuffling walk or loss of walking altogether
Other common clues
- Breathing irregularities (deep sighs or brief pauses)
- Seizures, which can range from subtle facial twitching to full convulsions
- Gastrointestinal problems like constipation and reflux
- Sleep disturbances, especially frequent nighttime awakenings
Facial features
While theres no single Rett face, many families notice a slightly higherarched palate and a subtle, somewhat grim expression when the child concentrates. These arent diagnostic, but they sometimes help clinicians piece the puzzle together.
Seeing it in pictures
Publicly available, responsibly sourced can give you a visual sense of early handwringing, gait changes, and facial cues. Just remember that every childs journey is unique.
Diagnosis process
Diagnosing Rett syndrome isnt about a single blood test; its a blend of clinical observation and genetic confirmation.
Clinical criteria
Doctors look for four stages:
- Early onset stagnation (06months): slowed growth of head circumference.
- Rapid regression (618months): loss of skills, handwringing, breathing issues.
- Plateau (210years): some improvement, though core deficits remain.
- Late motor deterioration (after 10years): increased rigidity, possible scoliosis.
Genetic testing
A blood or saliva sample is sent for DNA sequencing to check for MECP2, CDKL5, or FOXG1 mutations. Positive results confirm the diagnosis, while a negative test doesnt entirely rule it outclinical judgement still matters.
Differential diagnosis
Because the regression can look like autism, cerebral palsy, or even severe developmental delay, doctors compare key signs. Below is a quick sidebyside:
| Condition | Key distinguishing sign |
|---|---|
| Autism | Typically no loss of previouslylearned hand skills |
| Cerebral palsy | Static motor impairment from birth, not regression |
| Rett syndrome | Handwringing + rapid loss of speech after 6months |
Life expectancy
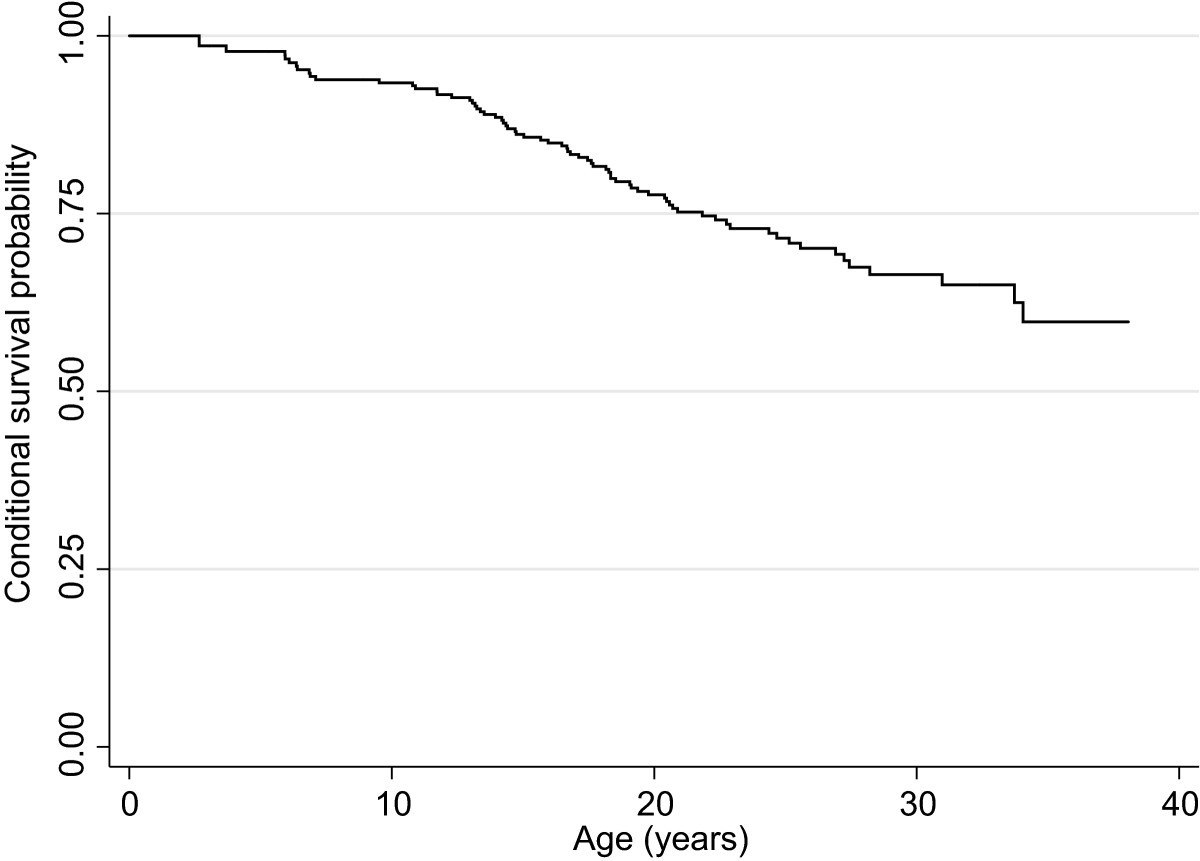
Thanks to multidisciplinary care, many girls with Rett now live well into their 40s and even 50s. A recent cohort study showed median survival of around 45years, with the majority reaching adulthood.
What influences longevity?
- Control of seizuresuncontrolled epilepsy is a major risk factor.
- Respiratory healthfrequent apnea episodes can be lifethreatening if unmanaged.
- Cardiac monitoringsome patients develop arrhythmias that need attention.
- Overall quality of supportive therapies (physical, occupational, speech).
In a , researchers emphasized that proactive, teambased care dramatically improves both lifespan and daytoday quality of life.
Treatment options
Theres no cure yet, but a toolbox of interventions can help manage symptoms and boost independence.
Standard medical care
- Antiseizure medications tailored to each childs seizure type.
- Physical therapy to maintain joint range of motion and prevent contractures.
- Occupational therapy focusing on hand functionadaptive tools can make a world of difference.
- Speech therapy that often shifts toward augmentative and alternative communication (AAC) devices.
Emerging therapies
Scientists are exploring genetherapy approaches that aim to deliver a functional copy of MECP2 directly into the brain. Earlyphase trials show promise, but theyre still experimental. Keeping an eye on updates from major research centers (like UCDavis) can help families stay informed about enrollment opportunities.
Supportive interventions
- Nutrition counselingmany children need highercalorie diets or feeding tubes.
- Breathing support, ranging from nighttime oxygen to occasional ventilator assistance.
- Behavioral strategies to address anxiety, meltdowns, or sensory sensitivities.
Quick weekly schedule (example)
- Monday & Wednesday: Physical therapy (45min)
- Tuesday: Speech/ AAC session (30min)
- Thursday: Occupational therapy (45min)
- Friday: Familyguided sensory play (1hour)
Real experiences
Facts are essential, but hearing a story can turn abstract data into something tangible.
Parent story
When our daughter Emma was 12months old, she suddenly stopped smiling at us, says one mother, and the handwringing started. It felt like watching a bright light dim. The diagnosis was a shock, but the moment the team explained that there are therapies that can give her back moments of joylike using a tablet to talkgave us hope we never imagined.
Clinician perspective
Dr. Patel, a pediatric neurologist, emphasizes, Managing seizures is the cornerstone. When we get those under control, families report dramatic improvements in sleep, mood, and overall interaction.
Practical toolbox
Downloadable symptomtracking sheets (available on the Rett Syndrome Research Trust website) can help you log daily changes, making conversations with clinicians more focused.
Find reliable info
With the internet full of mixedquality content, its vital to know where to turn for trustworthy guidance.
Trusted medical sites
Advocacy organizations
- Rett Syndrome Research Trust
- International Rett Syndrome Association
- Local support groupsmany meet virtually, offering a bridge between families across the globe.
Spotting misinformation
Ask yourself these quick questions before accepting a claim:
- Is the source a recognized medical institution or peerreviewed journal?
- Does the article cite uptodate research (ideally within the last five years)?
- Are the recommendations consistent with what your healthcare team says?
Conclusion
Rett syndrome is a rare, challenging condition that overwhelmingly affects girls, but with early detection, coordinated care, and a supportive community, many families find a path to a richer, fuller life. Understanding the genetics, spotting the early signs, and staying on top of treatment options are all part of empowering you to make informed choices. If youve learned something new, have a question, or just want to share your own journey, please leave a comment below. Lets keep the conversation goingbecause together were stronger, smarter, and, most importantly, more hopeful.
FAQs
What are the earliest signs of Rett syndrome in girls?
Typical early signs appear between 6‑18 months and include loss of purposeful hand skills, hand‑wringing, reduced speech, and gait abnormalities.
How is Rett syndrome diagnosed?
Doctors use clinical criteria (regression stages) plus genetic testing for MECP2, CDKL5, or FOXG1 mutations to confirm the diagnosis.
Can boys have Rett syndrome?
Boys can have Rett‑like conditions, usually when they have mosaic MECP2 mutations or larger chromosomal anomalies, but classic Rett overwhelmingly affects females.
What treatments improve quality of life for females with Rett?
Management focuses on seizure control, physical/occupational therapy, speech therapy with AAC devices, nutrition support, and breathing assistance when needed.
What is the current life expectancy for females with Rett syndrome?
With multidisciplinary care, many females live into their 40s‑50s; proactive management of seizures, respiratory health, and cardiac monitoring is crucial.