At first, I thought it was nothing then the headaches came, the confusion, the fear that something far worse was happening. If youve just learned that acute myeloid leukemia (AML) has reached the central nervous system (CNS), the most pressing question is: what does this mean for my survival and treatment? Below youll find a straightforward, compassionate guide that cuts straight to the answers you need, without any fluff.
Quick Answer Overview
What is the typical survival outlook?
For adults whose AML spreads to the CNS, median overall survival hovers around 23months, with a 2year survival rate of roughly 24% in recent series (see Haematologica 2023). Children fare a bit better; many pediatric studies show CNS involvement doesnotindependently shorten survival.
Does CNS disease change the treatment plan?
Yes. Alongside standard induction chemotherapy, doctors add intrathecal (spinalfluid) therapy and often highdose cytarabine to reach the brain and spinal cord. Routine CNS prophylaxis isnt recommended for everyone, only for those at high risk (see the ).
CNS Involvement Basics
How common is CNS disease in AML?
Only about 15% of adults present with CNS leukemia at diagnosis, but the rate climbs in relapsed or refractory cases and in certain cytogenetic subtypes such as monosomal karyotype.
What symptoms should raise alarm?
- Persistent or worsening headache
- Seizures, visual changes, or facial weakness
- Sudden confusion or difficulty speaking
- Unexplained blood in the cerebrospinal fluid (CSF)
These signs often overlap with more benign conditions, which is why a lumbar puncture (spinal tap) is essential for a definitive diagnosis. In a similar vein, for patients facing other complex conditions such as prostate removal life expectancy, understanding clinical markers and symptoms is crucial for prognosis and treatment planning.
How is CNS involvement diagnosed?
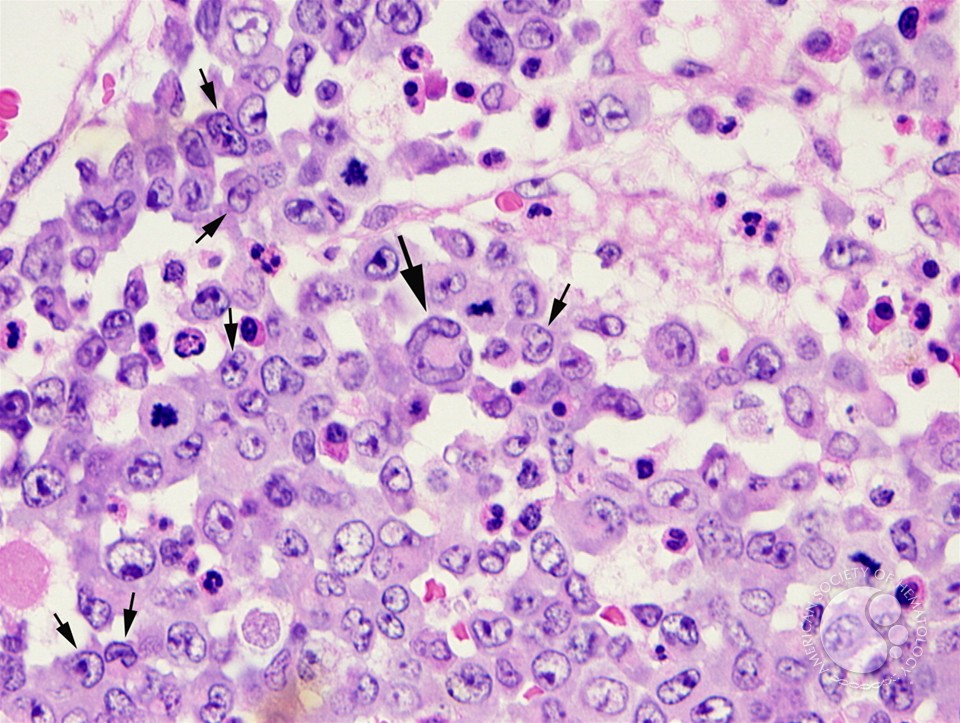
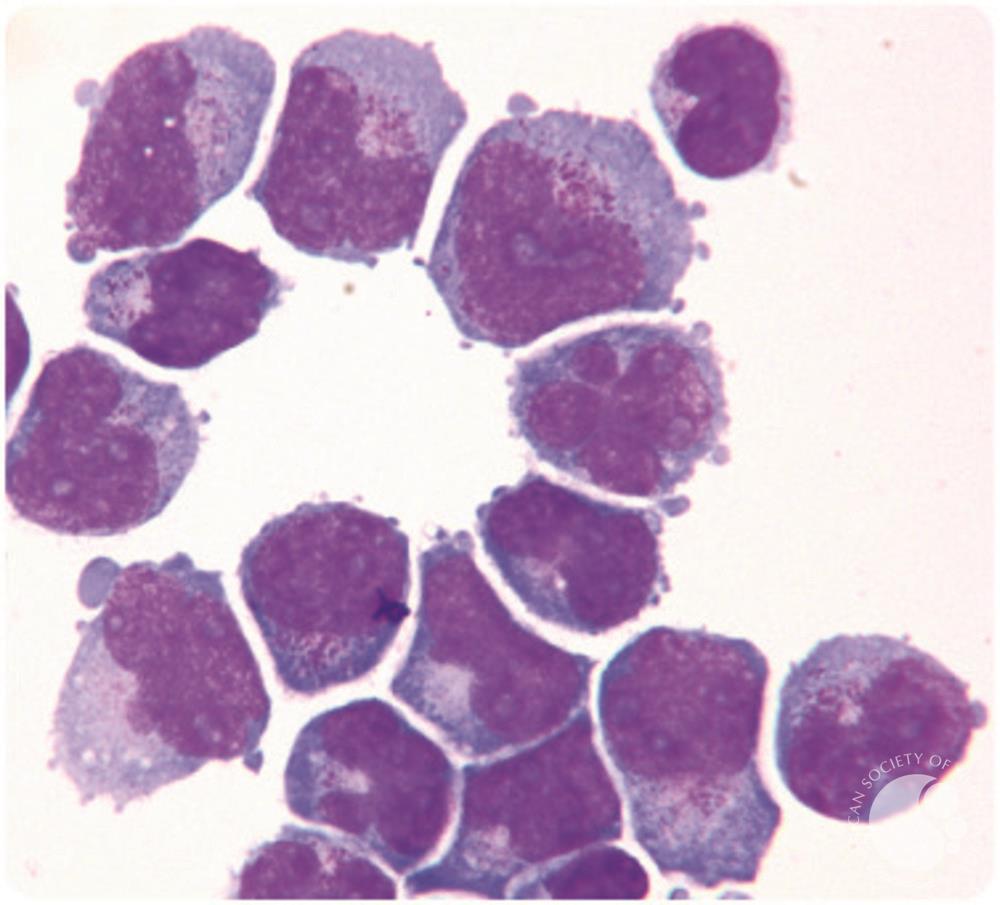
The gold standard is a lumbar puncture with cytology and flow cytometry to detect leukemic blasts in the CSF. Imaging, especially contrastenhanced MRI, can reveal leptomeningeal enhancement or parenchymal lesionswhat radiologists call AML brain radiology.
Prognosis Snapshot Overview
What does the latest research say?
Large cohort analyses report a median overall survival of 23months for adults with CNS disease, while 2year survival hovers around 24%. Children, in contrast, often show no statistically significant difference compared with CNSnegative peers.
Which subgroups have better or worse outcomes?
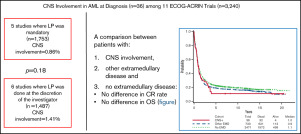
- Transplanteligible patients who achieve CNS clearance before hematopoietic stemcell transplant (HSCT) can see 3year survival rates climb to 11% versus 0% without transplant.
- Concurrent extramedullary disease (EMD) drops median survival further, sometimes to 11months.
- High whitecell count at diagnosis and monocytic morphology (FABM5) flag a higher risk of CNS spread.
Leukemia in brain versus CNS leukemia?
AML brain metastasis usually refers to solid parenchymal lesions, while CNS leukemia denotes leptomeningeal (spinalfluid) infiltration. Parenchymal lesions often signal a more aggressive disease and portend a shorter survival.
| Population | Median OS (months) | 2Year Survival | Key Source |
|---|---|---|---|
| Adults CNSpositive | 23 | 24% | Haematologica 2023 |
| Pediatrics CNSpositive | Not significantly different | 45% | Journal of Pediatric Hematology |
| Adults CNSnegative (baseline) | 1215 | 40% | ELN 2022 Report |
Treatment Landscape Overview
Standard therapy for AML with CNS involvement
Typical induction combines the 7+3 regimen (seven days of cytarabine plus three days of an anthracycline) with intrathecal cytarabine or methotrexate administered on days 1, 8, and 15. Highdose cytarabine (3g/m) is favored because it penetrates the CSF better than standard doses.
Targeted and novel agents (20232024)
FLT3 inhibitors (midostaurin, gilteritinib) dramatically improve systemic control, yet their CSF penetration remains limited. Early case series suggest venetoclaxbased combinations may cross the bloodbrain barrier, but robust data are still pending.
When is CNS prophylaxis considered?
Routine prophylaxis for all AML patients isnt supported by the evidence. However, highrisk featuresmonocytic AML (FABM5), whitecell count >10010/L, or prior CNS diseaseprompt many clinicians to add intrathecal therapy during induction.
Emerging approaches & clinical trials
Investigators are testing intrathecal CART cells (PhaseI, NCT05432112) and CNSdirected radiotherapy for bulky leptomeningeal disease. While still experimental, these strategies highlight the fields commitment to improving the grim prognosis.
Living With CNS AML
Redflag symptoms you shouldnt ignore
If you notice any sudden neurologic changebe it a new seizure, a sharp headache that wont ease, or visual disturbancescall your oncologist or go to the emergency department immediately.
How often should CSF be checked?
Most treatment protocols recommend a baseline lumbar puncture, another after the induction phase, and then every 23weeks until the CSF is clear of blasts.
Supportive care & qualityoflife tips
- Steroids (e.g., dexamethasone) can reduce cerebral edema and relieve headache.
- Seizure prophylaxis with levetiracetam is common for patients with leptomeningeal disease.
- Physical and occupational therapy help maintain mobility and independence.
- Psychological counseling or support groups can ease the emotional burdentalking to others who get it makes a massive difference.
Family planning and survivorship
Before starting intensive chemotherapy, discuss fertility preservation options (egg or sperm banking). For those who achieve remission, longterm neurocognitive monitoring is advised, as chemotherapy and intrathecal drugs can affect memory and processing speed.
Key Takeaways Summary
Bottom line: When AML reaches the CNS, the outlook becomes considerably tougher, with median survival measured in months for most adults. Early recognition of neurologic symptoms, prompt CSF analysis, and an aggressive treatment planincluding intrathecal therapy and, when possible, stemcell transplantationcan modestly improve odds.
What you can do now: Talk openly with your hematologyoncology team about intrathecal chemotherapy, transplant eligibility, and any clinical trials that might suit you. Stay vigilant for neurologic changes, and dont hesitate to reach out for supportive serviceswhether its a social worker, a therapist, or a patientpartner group.
If you or a loved one is navigating this journey, remember youre not alone. Share your experiences in the comments, ask any lingering questions, and consider downloading our to keep track of appointments, symptoms, and treatment milestones.
FAQs
What is the typical overall survival for adults with AML that has spread to the CNS?
Median overall survival for adults with CNS‑positive AML is about 2‑3 months, with a 2‑year survival rate near 24 % in recent series.
How does CNS involvement change the standard AML treatment plan?
In addition to conventional induction (7+3), patients receive intrathecal chemotherapy (cytarabine or methotrexate) and often high‑dose cytarabine to achieve adequate drug levels in the cerebrospinal fluid.
Which patients are considered high‑risk for CNS disease and might need prophylaxis?
High‑risk features include monocytic AML (FAB M5), white‑cell count > 100 × 10⁹/L, certain cytogenetic abnormalities, and a prior history of CNS involvement.
Can a stem‑cell transplant improve outcomes for CNS‑positive AML?
Yes. Patients who clear leukemic blasts from the CSF and then undergo hematopoietic stem‑cell transplantation can achieve 3‑year survival rates around 11 %, markedly better than without transplant.
What neurologic symptoms should prompt an urgent lumbar puncture?
New or worsening headaches, seizures, visual changes, facial weakness, sudden confusion, or any unexplained neurologic decline should trigger immediate CSF evaluation.