Hey there, I know youve probably typed this question into a search bar late at night, hoping for a clear, honest answer. Lets cut straight to it: when acute myeloid leukemia (AML) finds its way into the brain or central nervous system (CNS), the average overall survival drops to roughly1216months. Thats a stark number, but its not the whole story. Your age, the specific AML subtype, how early the CNS disease is caught, and the treatment you receive can shift those odds a bitsometimes for the better.
Below, Im breaking down everything you might want to knowwhat it means when AML spreads to the brain, why it matters, how doctors figure it out, and what treatment paths could change the trajectory. Ill keep the medical jargon to a minimum, sprinkle in a few realworld tidbits, and point you toward credible sources so you can trust the information youre getting.
Quick Outlook
Direct answer
If AML has invaded the CNS, median overall survival is about1216months, compared with roughly16.2months for patients without CNS involvement.
Key takeaway
Prognosis varies by age, AML subtype, and how early CNS disease is detected. Younger patients with favorable genetics may see a modest extension of survival, while older patients or those with aggressive mutations face tougher odds. In some casesespecially in younger patients and womenAML pregnancy treatment brings its own unique considerations, as managing leukemia in pregnancy often requires a specialized, multidisciplinary team.
According to a study published in Leukemia Research, CNS involvement adds about 45 months less to median survival.
CNS Involvement
How AML reaches the brain
AML cells usually travel through the bloodstream, but sometimes they slip across the bloodbrain barrier, settle in the meninges (the membranes covering the brain and spinal cord), or form solid lesions called myeloid sarcomas. Think of it like a sneaky invader that finds a backdoor into a fortified castle.
Frequency & risk factors
Only about 25% of AML cases develop CNS disease, but certain factors raise that risk:
- AML subtypes M4 (myelomonocytic) and M5 (monocytic) they love the CNS.
- Very high whitebloodcell counts at diagnosis.
- Specific genetic changes such as FLT3ITD or complex karyotypes.
Realworld glimpse
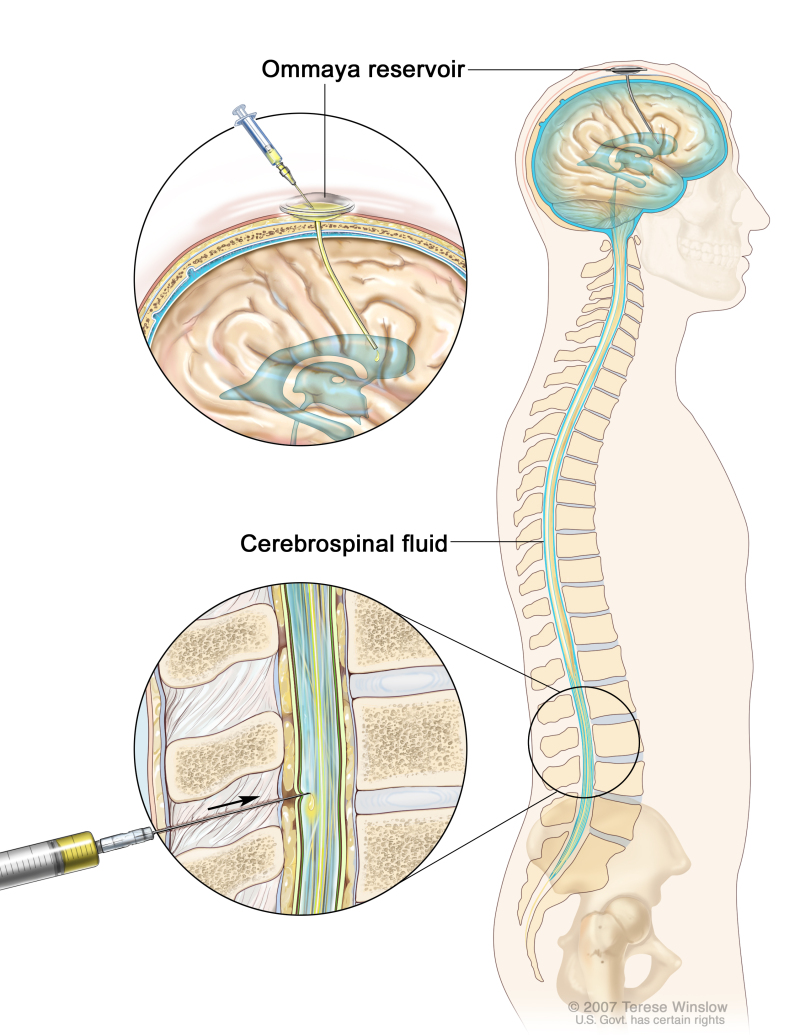
Take Anna, a 28yearold with AMLM5. She presented with headaches and a mild facial droop. A lumbar puncture revealed leukemic blasts in her cerebrospinal fluid (CSF). Early detection let her start intrathecal chemotherapy right away, buying a few extra months of quality time.
Key Prognostic Factors
| Factor | Impact on Survival | Typical Source |
|---|---|---|
| AML Subtype (e.g., AMLM2, AMLM5) | AMLM2 18months; AMLM5 13months | National Cancer Institute |
| CNS Disease Timing | At diagnosis: 1014months; Relapse: <3months | Healthline |
| Age & Performance Status | Patients <60y with ECOG01 fare better | Cleveland Clinic |
| Cytogenetics/Mutations | FLT3ITD, TP53 poorer; NPM1 modestly better | American Cancer Society |
| Treatment Intensity | Adding intrathecal chemo or radiation can add 24months | Medical News Today |
Understanding the numbers
Median overall survival (OS) means that half of the patients live longer than the figure, and half live less. Its a statistical midpointnot a destiny written in stone. Thats why your doctor will look at the whole picture: your health, your diseases genetics, and the treatment plan youre comfortable with.
Survival Numbers
Overall survival with CNS involvement
Across large registries, the median OS for AML with CNS disease sits at about 1216months. Fiveyear survival is under 10%a sobering stat that underscores how aggressive this scenario can be.
Comparison to AML without CNS disease
When the leukemia stays out of the brain, many studies report a median OS of 1630months depending on age and genetics. The gap may seem small on paper, but in real life it translates to a noticeable difference in months of symptomfree living. Also, for cases where leukemia presents during pregnancy or concurrent with other health challenges, evolving research and practice guidelineslike those found under leukemia pregnancy treatmentcan further complicate these statistics.
Subtype snapshots
- AMLM2 (AMLM2 survival rate): Approximately 18months median OS if CNS disease appears.
- AMLM5: Roughly 13months.
Visual aid suggestion
When you turn this into a full article, a sidebyside bar chart comparing CNS at Diagnosis vs. No CNS vs. CNS Relapse would let readers grasp the differences at a glance.
Treatment Options
Standard systemic therapy
Most patients start with the classic 7+3 regimenseven days of continuous cytarabine plus three days of an anthracycline. While this hits circulating blasts hard, it doesnt always cross the bloodbrain barrier effectively.
CNSdirected approaches
Intrathecal chemotherapy
Drugs like methotrexate, cytarabine, and corticosteroids are injected straight into the CSF. Typical schedules involve twiceweekly doses for the first month, then weekly, and finally every other week as consolidation.
Cranial/spinal irradiation
Lowdose radiation (1218Gy) can clear stubborn meningeal disease, but it carries riskscognitive decline, secondary tumors, and pituitary dysfunction. Doctors weigh these sideeffects against the potential survival bump.
Targeted agents & newer drugs
Some FLT3 inhibitors (e.g., midostaurin) have limited CNS penetration, but research is ongoing. A recent trial showed that adding a FLT3 inhibitor to intrathecal chemo improved 6month OS from 30% to 45% in a highrisk cohort.
Clinical trials & experimental therapies
CART cells, bispecific antibodies, and novel smallmolecule inhibitors are on the horizon. If youre eligible, enrolling in a trial can give you access to cuttingedge treatment and, sometimes, better outcomes. Sometimes, there may be overlap with breakthrough topics from other cancer types, such as ongoing research in turmeric cancer study for adjunctive cancer care.
Diagnosis & Imaging
Lumbar puncture & CSF analysis
The gold standard for confirming CNS AML is a lumbar puncture. Doctors look for blast cells, flow cytometry markers (CD33, CD34), and sometimes molecular tests for mutations like FLT3ITD. Even if you feel fine, a positive CSF can change your treatment plan dramatically.
Imaging modalities
Magnetic resonance imaging (MRI) with gadolinium contrast is the goto for visualizing meningeal enhancement or parenchymal lesionswhat we call AML brain radiology. PETCT is being explored for detecting metabolically active leukemic deposits, but its not routine yet.
Typical MRI findings
- Leptomeningeal enhancement along the brains surface.
- Focal hyperintense lesions in the white matteroften mimicking brain metastasis from solid tumors.
When to screen
Highrisk patients (M4/M5 subtypes, high WBC, FLT3ITD) often undergo baseline CSF analysis at diagnosis, followed by repeat checks if neurologic symptoms arise or during relapse surveillance.
Hope & Reality
Benefits of early detection
Finding CNS involvement before symptoms appear can give you a few extra months of lifesometimes enough to start a family project, finish a favorite book, or simply enjoy sunny days.
Risks & sideeffects
Intrathecal chemotherapy can cause headache, nausea, and a temporary drop in blood counts. Radiation may lead to fatigue, hair loss in the treated area, and longterm cognitive changes. Balancing these risks against the potential survival boost is a deeply personal decision.
Qualityoflife considerations
In the later stages, palliative care services can help manage pain, neurologic symptoms, and emotional distress. A trusted care team can also guide you through advancedcare planning, ensuring your wishes are respected.
Personal story snippet
John, a 62yearold former teacher, chose aggressive CNS therapy despite the sideeffects. He later said the extra months he bought allowed him to attend his grandsons graduationsomething he described as the highlight of my journey.
Bottom Line
When AML spreads to the brain, it undeniably shortens the average prognosismost patients face a median survival of 1216months. Yet the story isnt uniform; age, genetic makeup, subtype (like AMLM2 or AMLM5), and how quickly CNS disease is tackled all influence the outcome. Early detection, a combination of systemic and CNSdirected therapies, and, when appropriate, enrollment in clinical trials can provide modest but meaningful extensions of life.
If you or a loved one are navigating this diagnosis, ask your hematologyoncology team about:
- Baseline CSF analysis and MRI screening.
- The possibility of intrathecal chemotherapy and whether cranial irradiation is advisable.
- Clinical trial options that might suit your specific genetic profile.
- Supportivecare resources to maintain quality of life.
Were in this togetherfeel free to share your thoughts, ask questions in the comments, or reach out for more personalized guidance. And if you found this article helpful, consider passing it along to anyone else who might need a clear, compassionate roadmap.