When leukemia cells make their way into the fluid that cushions your spine, the whole picture changes. Suddenly you might notice headaches, balance problems, or even seizures signs that the disease has entered the central nervous system (CNS). Those symptoms are a red flag that more aggressive, spine-focused treatment may be needed, and they can affect survival odds.
Understanding whats happening, why it matters, and what you can do about it isnt just medical trivia its a roadmap for staying one step ahead and feeling a little more in control during an overwhelming time.
Understanding CNS Involvement
What is leukemia in spinal fluid?
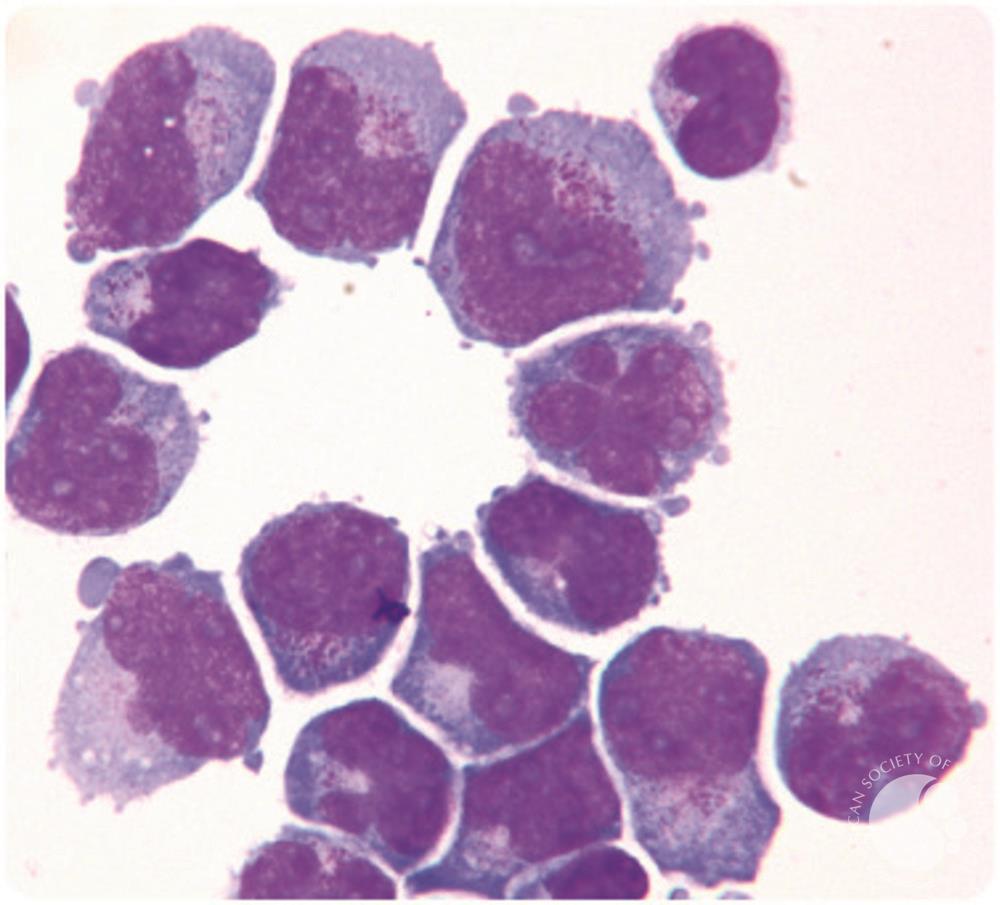
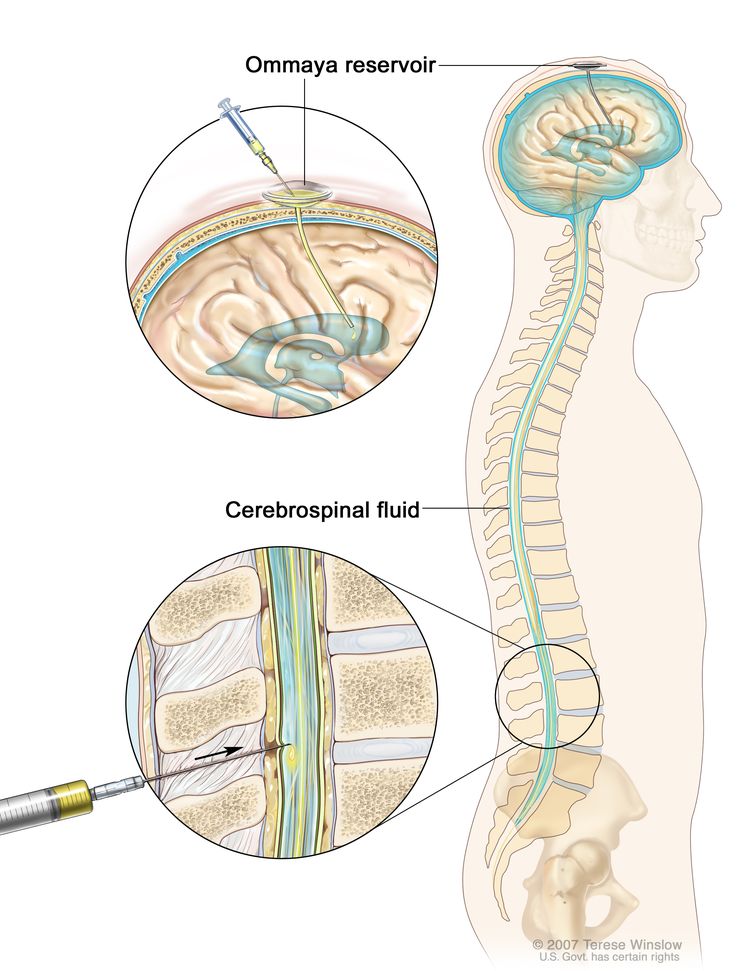
The spinal fluid, or cerebrospinal fluid (CSF), is a clear liquid that bathes the brain and spinal cord, protecting them like a cushion. When leukemic blasts slip into this fluid, doctors call it leukemia in the spinal fluid. It means the cancer has crossed the blood-brain barrier and is now lurking where it can affect nerve function.
How does leukemia reach the spine?
Leukemia spreads to the CNS in a few ways. The most common route is hematogenous spread cancer cells travel through the bloodstream and infiltrate the meninges, the thin membranes surrounding the brain and spinal cord. Sometimes, the disease directly breaches the meningeal layer, especially in aggressive subtypes. Think of it like a tiny invader finding a hidden backdoor into a heavily guarded castle.
Difference between spinal and brain spread
Both the spine and brain are part of the CNS, but they give you different warning signs. Spinal involvement often starts with back pain, neck stiffness, or trouble walking, while brain involvement might first show up as headaches, visual changes, or seizures. The prognosis can also differ; historically, brain involvement has been linked to slightly lower survival rates, but modern therapies are narrowing that gap.
What does it mean when leukemia is in the spinal fluid?
In plain language, it means the disease has taken a shortcut into the central nervous system, which can make it harder to clear with standard chemotherapy alone. Its a signal to your medical team that youll need treatments that travel directly into the CSF.
What happens when leukemia spreads to the brain?
- Persistent headaches
- Vision disturbances
- Seizures or confusion
- Potential longterm cognitive effects
Spinal Symptoms Overview
Common early clues
Early signs are often subtle, but they shouldnt be ignored. You might feel a dull ache in the lower back, a feeling of heaviness in the legs, or occasional nausea that doesnt have an obvious cause. Some people notice a sensation of tightness around the head that feels like a band.
Red-flag symptoms that need urgent care
If you experience any of the following, call your doctor right away:
- Sudden, severe headache that wakes you up at night
- Unexplained weakness or numbness in arms or legs
- Loss of bladder or bowel control
- Sudden vision loss or double vision
- Any seizure activity, even if its brief
How symptoms differ in children vs. adults
Kids often cant articulate what theyre feeling, so you may notice behavioral changes irritability, increased sleepiness, or a sudden decline in school performance. Adults, on the other hand, tend to report more classic neurologic complaints like balance issues or persistent pain.
Real-world example: a teens first seizure
Emily, a 16-year-old diagnosed with ALL, began having occasional headaches that she brushed off as school stress. One evening she had a brief seizure while doing homework. Her neurologist ordered a lumbar puncture, which revealed leukemic cells in her CSF. The early detection allowed her team to start intrathecal chemotherapy immediately, dramatically improving her outlook.
Diagnosis Process Steps
Lumbar puncture (spinal tap) what to expect
The gold standard for confirming CNS involvement is a lumbar puncture. Youll lie on your side, a local anesthetic is applied, and a thin needle is inserted between the lower back vertebrae to draw a small amount of CSF. The fluid is then examined under a microscope for leukemic blasts. The procedure sounds scarier than it is, and most patients report just a brief pressure sensation.
Imaging & lab tests
In addition to the spinal tap, doctors often order an MRI of the spine and brain. MRI can show subtle meningeal enhancement a sign of inflammation that sometimes accompanies leukemic infiltration. Blood tests, including flow cytometry, help identify the specific leukemia subtype, which guides treatment choices.
Interpreting results: leukemia in spinal fluid survival rate
Recent data suggest that patients with CNS-positive leukemia have a 5-year survival rate ranging from 7080% for ALL and 4050% for AML when treated with modern CNS-directed therapies. Early detection via lumbar puncture significantly boosts those numbers. For patients also navigating pregnancy, specialized approaches such as AML pregnancy treatment may be needed to balance maternal and fetal safety while treating CNS disease.
Comparison table Survival rates
| Leukemia Type | CNS-Positive 5-Year Survival | Standard Treatment |
|---|---|---|
| Acute Lymphoblastic Leukemia (ALL) | 7080% | Intrathecal chemo + systemic high-dose chemo |
| Acute Myeloid Leukemia (AML) | 4050% | Intrathecal chemo + targeted agents |
Treatment Options Overview
Intrathecal chemotherapy
This is the cornerstone for CNS disease. Drugs like methotrexate, cytarabine, or hydrocortisone are injected directly into the CSF, bypassing the blood-brain barrier. The schedule usually involves several weekly doses followed by maintenance cycles.
Systemic high-dose chemotherapy & targeted agents
When the disease is aggressive, doctors add high-dose systemic chemo that can penetrate the CSF to a degree. For certain genetic mutations, targeted therapies such as tyrosine-kinase inhibitors (TKIs) are also effective and have fewer side effects than traditional chemo.
Radiation therapy to the spine
Radiation is reserved for cases where chemotherapy isnt enough or when theres rapid neurological decline. It can shrink meningeal disease but carries risks like long-term spinal growth issues in children, so its used judiciously.
Emerging therapies & clinical trials (2025)
Hope is on the horizon. CAR-T cell therapy, which engineers a patients own immune cells to hunt leukemic blasts, is being tested for CNS disease. Small-molecule inhibitors that cross the blood-brain barrier are also showing promise in early trials.
Decision-making flowchart What treatment for my situation?
- Confirm CNS involvement with lumbar puncture.
- Identify leukemia subtype (ALL vs. AML).
- Start intrathecal chemotherapy immediately.
- Assess response after 23 cycles.
- If inadequate, discuss adding high-dose systemic chemo, targeted agents, or enrollment in a clinical trial.
Prognosis & Survival Outlook
Overall survival when leukemia reaches the CSF
The short answer: its serious, but not a death sentence. Survival hinges on how early the CNS disease is caught and how aggressively its treated. With diligent therapy, many patients achieve long-term remission.
Factors that improve outcomes
- Early detection via routine CSF checks.
- Younger age (children often respond better to CNS-directed therapy).
- Leukemia subtype ALL generally fares better than AML.
- Complete response to intrathecal chemotherapy.
- Access to clinical trials offering cutting-edge treatments.
Long-term followup & quality of life
Even after remission, survivors need regular neurologic exams, MRI scans, and CSF monitoring to catch any relapse early. Physical therapy can help restore strength and balance, while neurocognitive assessments address any subtle learning or memory issues that may have arisen.
Patient story navigating life after CNS involvement
Mark, a 42-year-old with AML, recalls the shock of learning his leukemia had entered his spinal fluid. After a series of intrathecal and high-dose treatments, he entered remission. Today, he participates in a weekly yoga class to keep his spine flexible and attends a support group where he shares his journey, providing hope for others walking the same road.
Frequently Asked Questions
What does it mean when leukemia is in the spinal fluid?
It signals that leukemic cells have infiltrated the cerebrospinal fluid, increasing the risk of neurological symptoms and necessitating CNS-directed therapy.
How is leukemia in spinal fluid diagnosed?
A lumbar puncture collects CSF for cytology and flow cytometry; imaging (MRI) may be added to assess the extent of involvement.
Can leukemia spread from person to person?
No. Leukemia is a blood-cell cancer that originates from mutations inside the body; it is not contagious.
What are the survival rates for leukemia in the brain vs. spine?
Studies show 5-year survival of 7080% for ALL with CNS involvement and 4050% for AML, with slightly lower numbers historically for brain involvement, though modern therapy is closing that gap.
What treatments are available for spinal CNS leukemia?
Intrathecal chemotherapy is the backbone, complemented by high-dose systemic chemo, targeted agents, radiation (in select cases), and emerging options like CAR-T cells.
Balancing Risks & Benefits
Benefits of aggressive CNS therapy
Higher remission rates, reduced risk of permanent neurologic damage, and a better chance at long-term survival. In many cases, early CNS control prevents future relapses that are far harder to treat.
Risks and side-effects to consider
Intrathecal chemo can cause headaches, nausea, and rare neurotoxicity. High-dose systemic chemo brings the usual risks of infection and organ strain. Radiation carries long-term concerns, especially in children, such as growth inhibition and secondary cancers.
Shared decision-making tools
Ask your oncologist these questions:
- What is my specific leukemia subtype and its CNS risk?
- How many intrathecal treatments will I need before we assess response?
- Are there clinical trials Im eligible for?
- What supportive care (physical therapy, counseling) is recommended?
Sample checklist Am I ready for intrathecal chemo?
- Do I understand the procedure and potential side-effects?
- Has my team explained the schedule and followup plan?
- Do I have a support system for transport and aftercare?
- Am I aware of signs that require urgent medical attention?
Conclusion
When leukemia spreads to the spine, it flips a switch that calls for swift, focused action. Early symptoms may be easy to miss, but recognizing them can lead to timely lumbar punctures, targeted intrathecal therapy, and a much brighter outlook. Survival rates are improving, especially for ALL, thanks to modern CNS-directed treatments and emerging trials. Balancing the benefits of aggressive therapy against potential side-effects is a personal journey best navigated with a trusted medical team and a strong support network.
If you or someone you love is facing this challenge, dont wait talk to your oncologist about CNS testing, explore all treatment options, and lean on community resources. Knowledge and early action are powerful allies in the fight against leukemia.
FAQs
What are the symptoms when leukemia spreads to the spine?
Common symptoms include back pain, neck stiffness, trouble walking, weakness or numbness in limbs, and sometimes loss of bladder or bowel control.
How is leukemia in the spinal fluid diagnosed?
Doctors use a lumbar puncture to collect spinal fluid and check for leukemia cells, often combined with MRI imaging for confirmation.
What treatments are used for leukemia in the spine?
Treatment typically includes intrathecal chemotherapy, high-dose systemic chemo, targeted agents, and sometimes radiation therapy.
Can leukemia in the spine be cured?
With early detection and aggressive treatment, many patients achieve remission, especially with modern CNS-directed therapies.
What is the survival rate for leukemia in the spinal fluid?
Survival rates vary: ALL has a 70-80% 5-year survival, while AML ranges from 40-50% with timely, targeted treatment.