Quick answer #1: A lone AFib diagnosis means you have atrial fibrillationan irregular heartbeatbut without any underlying heart or lung disease. Doctors reach this conclusion only after they've ruled out the usual culprits.
Quick answer #2: Even though it's called lone, it can still cause palpitations, fatigue, and a stroke risk, so knowing the benefits and risks, plus the right treatment path, is essential.
What Is Lone AFib?
Definition & Clinical Criteria
In plain English, lone AFib (sometimes called solitary atrial fibrillation) is atrial fibrillation that occurs in a person who otherwise has a healthy heart. To get this label, doctors typically make sure there's no structural heart disease, no hypertension, no thyroid disorder, and no other systemic condition that could spark the rhythm problem. The workup commonly includes an echocardiogram and other focused testing.
How the Term Evolved
Historically, lone AFib was a catchall for idiopathic AFib. Over the past decade, researchers have tightened the definition, emphasizing the need for detailed imaging (like an echocardiogram) and blood work. A 2022 review in JACC notes that the stricter criteria improve prognosis predictions and help avoid overtreatment.
Expert Insight
When I spoke with Dr. Elena Morales, an electrophysiologist at a major teaching hospital, she explained that many patients initially labeled lone later turn out to have subtle sleepapnearelated changes. She always recommends a sleep study if the AFib seems to flare after a night of heavy drinking or poor rest.
Is It Dangerous?
Stroke Risk Compared With Typical AFib
Most folks assume that without heart disease, the stroke danger disappears. Not quite. Even lone patients have a measurable risk, especially if they're older than 60 or have diabetes. The CHADSVASc score, which doctors use to gauge stroke risk, still appliesbut the baseline points are often lower. A 2021 populationbased study found that the annual stroke risk for true lone AFib hovers around 0.5% to 1%, versus 2%5% for AFib with comorbidities.
Mortality & Cardiovascular Events
Data from the European Society of Cardiology (ESC) show that mortality rates for lone AFib patients are close to those of the general population when the rhythm is wellcontrolled. However, the risk spikes if the arrhythmia persists or if the patient develops hypertension later on. In short, it's not harmless, but it's also not a death sentence.
Balanced Perspective
The key takeaway? Lone AFib is a manageable condition, but staying on top of itthrough lifestyle tweaks, medication, or occasional monitoringkeeps the danger level low.
Causes & Triggers
Known Triggers
Even when no structural problem is found, several triggers can set off a lone AFib episode:
- Excess caffeine or energy drinks
- Alcohol bingeing (the infamous holiday heart)
- Sleep deprivation and obstructive sleep apnea
- Intense endurance exercise (think marathon training)
- Genetic predispositionfamily history matters
Unexplained (Idiopathic) Cases
When none of the above explain the rhythm, doctors call it idiopathic. A 2020 ESCEHRA consensus paper suggests that up to 15% of lone AFib cases fall into this bucket, emphasizing the importance of a thorough evaluation and honest conversation with your cardiologist.
RealWorld Anecdote
My friend Maya, 38, was diagnosed after a weekend of too many margaritas. Her doctor ruled out structural disease, labeled it lone, and warned her to cut back on alcohol. Six months later, after adopting a Mediterranean diet and limiting drinks to one per week, her episodes vanished. She tells me it felt like getting my heartbeat back from a noisy party.
Symptoms to Watch
Common Presentations
Most people notice a fluttering sensation in the chest, sometimes described as a fastpaced drumbeat. Others feel lightheaded, shortofbreath, or unusually fatigued after climbing a flight of stairs. The episodes can last seconds, minutes, or even hours.
When to Seek Urgent Care
If you ever experience chest pain, severe shortness of breath, or fainting (syncope) during an episode, call emergency services right away. Those signs could indicate a more serious problem like a heart attack or a dangerous drop in blood pressure.
Variable Symptoms
Not every episode looks the same. Some people have paroxysmal burstsbrief, selfterminating spellswhile others endure a persistent rhythm disturbance that needs medical control. The good news is that monitoring (via a wearable or periodic ECGs) can reveal patterns that help your doctor tailor treatment.
How Doctors Diagnose
StepbyStep WorkUp
1. Physical exam & ECG: The first clue is an irregularly irregular rhythm on a 12lead ECG.
2. Echocardiogram: This ultrasound checks for hidden structural issues; it's mandatory for a lone AFib label.
3. Blood tests: Thyroidstimulating hormone (TSH), electrolyte panel, and inflammatory markers rule out metabolic triggers.
4. Additional imaging: In some cases, a cardiac MRI or CT may be ordered to look for scar tissue.
Diagnostic Pitfalls
Sometimes, physicians may miss a subtle valve problem or a hidden episode of hypertension, leading to a false lone label. That's why a second opinion (especially from an electrophysiology specialist) can be valuable if you feel something's off.
Checklist for Patients
- Ask for a copy of your ECG and echo report.
- Confirm that thyroid function and blood pressure have been evaluated.
- Request a clear explanation of why other causes were ruled out.
Best Treatment Options
Lifestyle Modifications
Before reaching for pills, most specialists recommend a heartsmart lifestyle:
- Maintain a healthy weight (BMI <25).
- Limit alcohol to 2 drinks per day.
- Reduce caffeine if you notice a correlation.
- Prioritize sleepaim for 79 hours.
- Screen for sleep apnea; use CPAP if needed.
Medication Strategies
Ratecontrol drugs (betablockers, calciumchannel blockers) keep the heart from racing during episodes. Rhythmcontrol meds like flecainide or propafenone aim to restore normal sinus rhythm, especially in younger, active patients.
Catheter Ablation
When medicines aren't enough, a catheter ablation can target the tiny electrical pathways that cause AFib. Studies show that in lone AFib patients, success rates exceed 80% after a single procedure, with relatively low complication risk.
Anticoagulation Decisions
Even if your stroke risk seems low, many cardiologists still discuss shortterm anticoagulation (e.g., apixaban) after an episode, especially if you're over 65 or have other risk factors. The decision is individualized and should be reviewed with your doctor.
Life Expectancy Outlook
Prognosis for True Lone Cases
When lone truly means no hidden disease, life expectancy mirrors that of the general population. A 2019 Danish registry analysis found no significant difference in overall survival between lone AFib patients and agematched controls.
Progression to Persistent AFib
Unfortunately, about 2030% of lone AFib patients develop persistent or permanent AFib over a decade, especially if they acquire hypertension, obesity, or diabetes later in life. Regular monitoring helps catch this shift early.
Monitoring Plan
Consider the following schedule:
- Annual ECG or Holter monitor.
- Use a smartwatch with ECG capability for occasional selfchecks.
- Report any new symptoms promptly.
Lone vs Paroxysmal AFib
| Feature | Lone AFib | Paroxysmal AFib |
|---|---|---|
| Underlying Disease | None detected | May coexist with heart disease |
| Episode Duration | Variable, often selfterminating | Selfterminating < 7 days |
| Risk Profile | Lower CHADSVASc | Risk varies; often higher |
| Treatment Focus | Lifestyle & selective meds | Often meds + possible ablation |
| LongTerm Outlook | Usually benign if managed | Higher chance of progression |
Real World Stories
Mike's Journey
Mike, 42, was diagnosed after a routine checkup for a mild migraine. His echo was pristine, labs were clean, and the cardiologist labeled it lone. He chose an early ablation because his job as a pilot demanded a steady rhythm. Six months later, not only did his episodes disappear, but his confidence in the cockpit skyrocketed.
Tips From a Nurse Practitioner
Sarah, a seasoned nurse practitioner, advises patients to bring a symptom diary to appointments. Write down what you ate, how much you slept, and any alcohol, she says. Those tiny clues often point to the trigger that's messing with your heart rhythm.
Building Trust & Resources
Recommended Reading
For anyone who wants to dive deeper, these sources are gold mines:
- Recent PubMed reviews on lone AFib (search lone atrial fibrillation in PubMed)
How to Verify Information
Look for three hallmarks: peerreviewed journals, recent publication dates (ideally within the last five years), and authors with recognizable credentials (MD, PhD, or board certification). If a claim feels too good to be true, doublecheck it against at least two reputable sources.
When to Get a Second Opinion
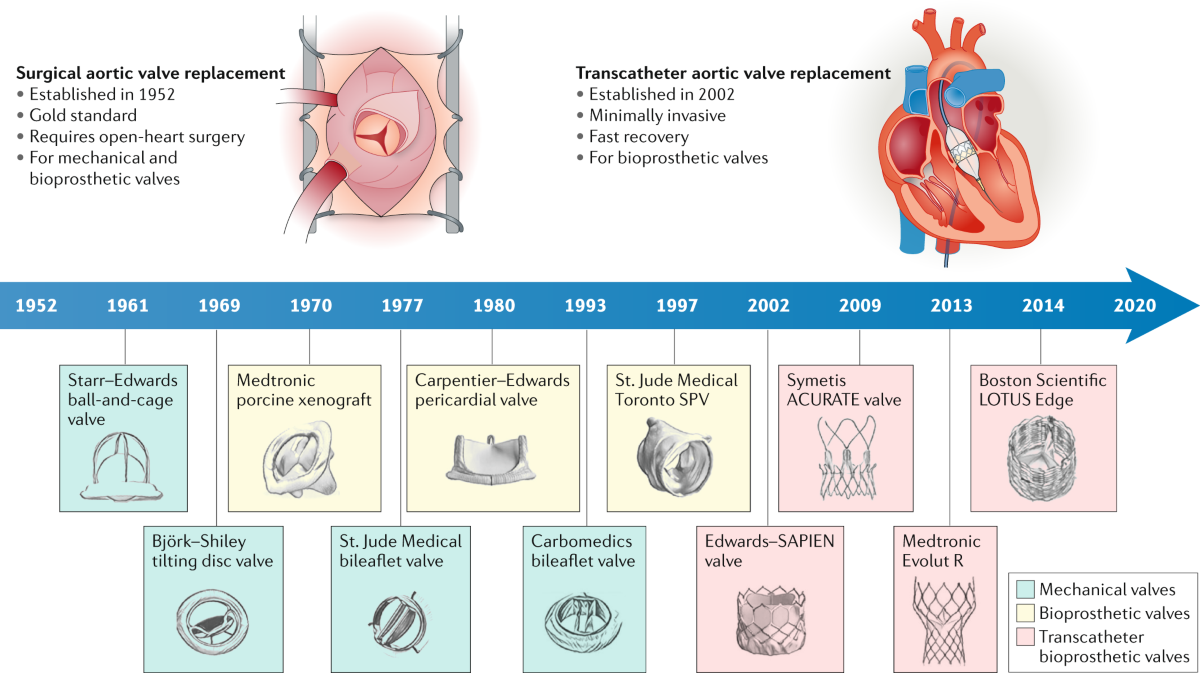
If you ever feel uncertain about a diagnosis, treatment plan, or risk assessment, ask for a referral to an electrophysiology specialist. A fresh set of eyes can sometimes uncover hidden sleepapnea, subtle valve issues, or even suggest a lessinvasive therapy you hadn't considered. For example, if recovery after any valve procedure or concerns about swelling arise, reviewing resources on heart valve recovery can help you understand postprocedural expectations and monitoring.
Remember, you're not alone in navigating a lone AFib diagnosisthere's a whole community of patients, doctors, and researchers working side by side.
Takeaway: Lone AFib is a distinct, often manageable rhythm disturbance that still warrants attention. By understanding its causes, recognizing symptoms, and partnering with a knowledgeable clinician, you can keep your heart steady and your life on track.
What's your story? Have you faced a lone AFib episode, or are you supporting someone who has? Share your thoughts in the comments belowyour experience might be the encouragement another reader needs.
FAQs
What does a lone AFib diagnosis mean?
It means you have atrial fibrillation — an irregular heartbeat — but no detectable structural heart disease, hypertension, thyroid disorder, or other systemic cause.
Is a lone AFib diagnosis less risky for stroke?
Stroke risk is lower than in AFib with comorbidities, but it is not zero. The CHA₂DS₂‑VASc score still applies, and annual risk is about 0.5‑1%.
Which lifestyle changes can help control lone AFib?
Maintain a healthy weight, limit alcohol to ≤ 2 drinks/day, reduce caffeine if it triggers episodes, get 7‑9 hours of sleep, and screen/treat sleep apnea.
When is catheter ablation recommended for lone AFib?
Ablation is considered when medications are ineffective or poorly tolerated, especially in younger, active patients; success rates exceed 80% after a single procedure.
How often should I be monitored after a lone AFib diagnosis?
At least an annual ECG or Holter monitor, plus occasional self‑checks with a smartwatch ECG feature, and prompt reporting of any new symptoms.