When your body is slammed with a major stressorthink severe infection, a big surgery, or a sudden traumayour bloodsugar can shoot up even if youve never been diagnosed with diabetes. This spike, known as stressinduced hyperglycemia in nondiabetics, isnt just a random lab number; it can change how you recover, how long you stay in the hospital, and even your longterm health outlook. Below, Im breaking it down the way I would explain it to a friend whos just heard the term and wants clear, practical answers.
What Is StressInduced Hyperglycemia?
Definition & diagnostic threshold
In plain language, stressinduced hyperglycemia (SIH) occurs when a nondiabetic persons blood glucose rises above 180mg/dL during an acute illness or injury. Doctors use this cutoff because its the point where the risk of complications starts to climb noticeably.
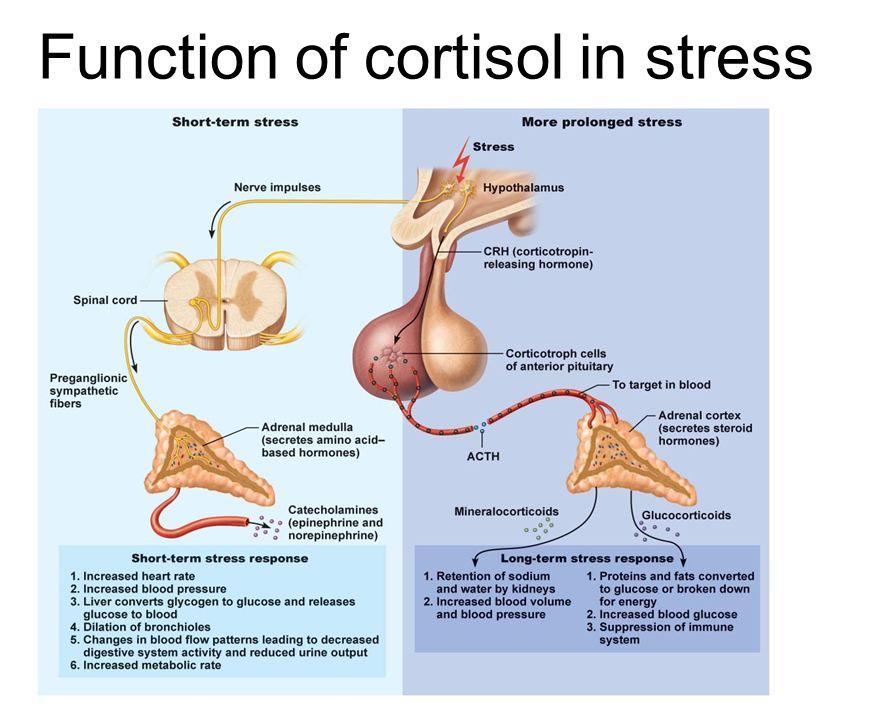
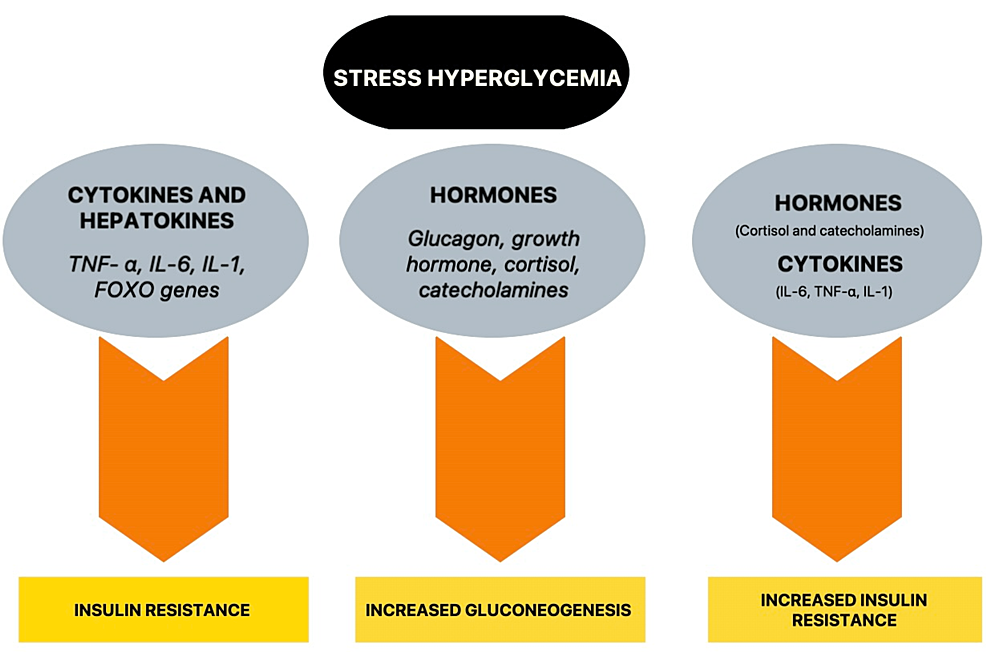
How the bodys stress response raises sugar
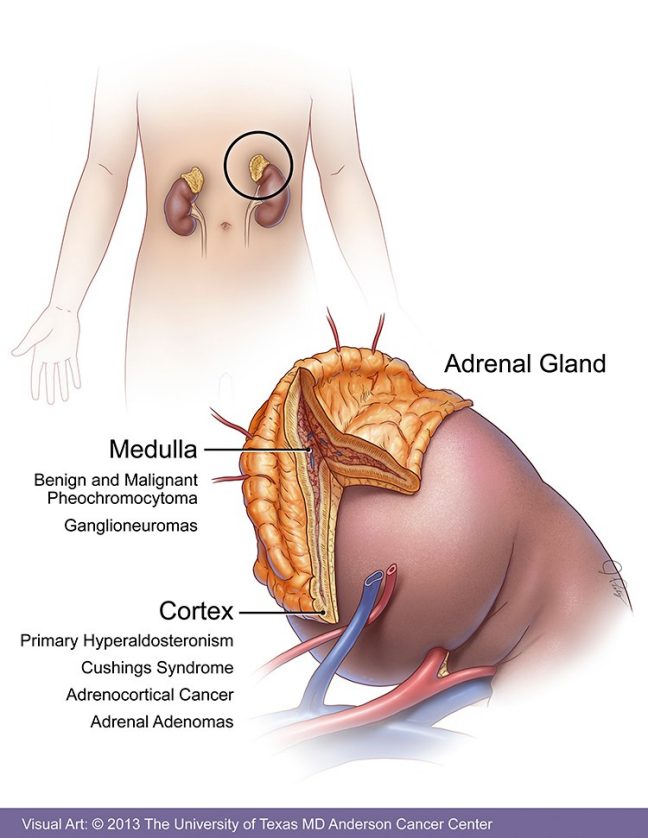
When youre under stress, your adrenal glands flood you with cortisol and catecholamines (like adrenaline). These hormones tell your liver, Hey, release more glucoseyour muscles might need extra fuel! At the same time, they make your cells a bit resistant to insulin, so the sugar stays in the bloodstream longer.
Common clinical settings
- Intensivecare admissions for heart attacks or strokes
- Severe infections such as pneumonia or urinarytract infections
- Major surgeries, especially orthopedic or cardiac procedures
- Trauma cases, burns, and severe blood loss
SIH vs. Typical Diabetes Hyperglycemia
| Feature | StressInduced Hyperglycemia | DiabetesRelated Hyperglycemia |
|---|---|---|
| Onset | Acute, within hours of stress | Chronic, progressive |
| Typical glucose range | 140300mg/dL (often >180) | Varies; can exceed 300mg/dL |
| Underlying issue | Hormonal surge temporary insulin resistance | Persistent cell dysfunction |
Who Gets SIH?
Epidemiology
Studies show that up to 50% of nondiabetic patients admitted with an acute myocardial infarction develop SIH ().
Major risk enhancers
- Age over 65
- Obesity or metabolic syndrome
- Prediabetes (elevated HbA1c but not yet diabetic)
- Severe physical trauma or burns
- Intense emotional stress (e.g., sudden loss, extreme anxiety)
StressHyperglycemia Ratio explained
The stresshyperglycemia ratio compares the admission glucose level to the estimated average glucose derived from a recent HbA1c. A ratio>1.8 often flags a true stress response rather than undiagnosed diabetes.
Spotting The Symptoms
Classic hyperglycemia signs
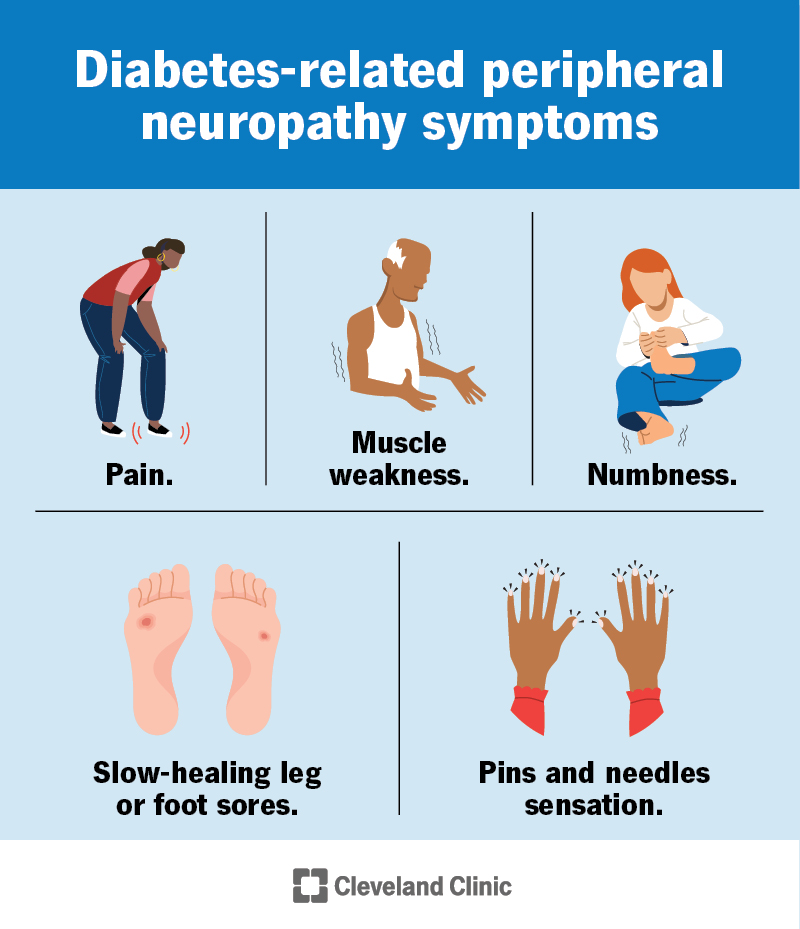
Even without diabetes, you might notice:
- Frequent urination (polyuria)
- Excessive thirst (polydipsia)
- Unexplained fatigue
- Blurred vision
Atypical or silent presentations
Many patients dont get the textbook symptoms. Instead, they may experience:
- Worsening infection or slower wound healing
- Confusion or delirium, especially in older adults
- Unexpected drops in blood pressure
When clinicians should suspect SIH
If a nondiabetic patients glucose spikes above 180mg/dL during an acute illness, its a red flag. Even a single reading of 190mg/dL in the emergency department warrants close monitoring. For patients with underlying endocrine issues, such as those being evaluated for primary hypothyroidism, teams should be extra vigilant because overlapping metabolic disturbances can complicate glucose control.
Why It Matters
Shortterm complications
Elevated glucose can impair whitebloodcell function, making infections harder to clear. It also increases the risk of dehydration and electrolyte disturbances.
Longterm outcomes
Patients with SIH have higher mortality rates after trauma or stroke. Moreover, about 15% of those who experience SIH develop overt diabetes within a year, underscoring the need for followup.
Balancing benefits & risks
Interestingly, a modest rise in glucose provides quick energy for the brain and heart. The challenge is keeping it from soaring into the dangerous range where blood vessels and nerves get damaged.
Managing SIH
Hospitalbased strategies
Most hospitals follow an insulinbased protocol:
- Target glucose <180mg/dL (preferably 140180mg/dL).
- Use a slidingscale or basalbolus regimen, depending on the patients stability.
- Check glucose every 46hours in the ICU, then daily as the acute stress resolves.
Nonpharmacologic measures
Address the root cause:
- Promptly treat infections with appropriate antibiotics.
- Ensure adequate hydration and nutrition.
- Provide pain control and early mobilization to reduce catecholamine spikes.
Postdischarge followup
After you leave the hospital, the work isnt over:
- Schedule an HbA1c test 3months later to see if glucose levels have normalized.
- Adopt a balanced dietthink whole grains, lean proteins, and plenty of vegetables.
- Incorporate regular lighttomoderate exercise, which improves insulin sensitivity.
Sample insulindosing algorithm
| Glucose (mg/dL) | Initial insulin dose | Adjustment every 2h |
|---|---|---|
| 180250 | 0.05U/kg IV bolus | +0.02U/kg if >250 |
| 250350 | 0.10U/kg IV bolus | +0.05U/kg if >350 |
| >350 | 0.15U/kg IV bolus | Add continuous infusion |
RealWorld Case Stories
Case study: Postop SIH in a senior patient
Mrs.L, a 72yearold who underwent hip replacement, had a glucose reading of 210mg/dL on postoperative day1. The orthopedic team started a lowdose basalbolus regimen and treated a lowgrade fever with antibiotics. Within 48hours, her glucose fell to 150mg/dL, and she was discharged home three days earlier than the average stay for similar cases.
Expert insight
Endocrinology fellow Dr.AnaMartinez notes, We often dismiss a glucose of 190mg/dL in a nondiabetic trauma patient, but early insulin and aggressive infection control can shave days off the ICU stay.
Patient voice
John, a 45yearold who was hospitalized for severe pneumonia, recalls, I thought that high sugar meant Id finally be diagnosed with diabetes. Turns out it was the infection. After the antibiotics and a short insulin course, my numbers went back to normal.
Bottom Line Checklist
- Recognize any glucose >180mg/dL in a nondiabetic during acute illness.
- Act quickly with insulin protocols and treat the underlying stressor.
- Monitor regularly while the patient is in the hospital.
- Followup after discharge with HbA1c testing and lifestyle guidance.
Stressinduced hyperglycemia may feel like an unwelcome surprise, but its a predictable part of the bodys fightorflight chemistry. By staying alert, treating the root cause, and using a balanced insulin approach, most people bounce back to normal glucose levels once the crisis passes. If youve ever seen a sudden sugar spike during a hospital stayor if youre caring for someone who hasask the care team about SIH and what monitoring plan they have in place. Got questions or personal experiences to share? Drop a comment below; were all in this together.
FAQs
What causes stress-induced hyperglycemia in non-diabetics?
Stress-induced hyperglycemia happens when severe illness, trauma, or emotional stress triggers hormone changes that raise blood sugar in people without diabetes.
How is stress-induced hyperglycemia diagnosed?
It’s diagnosed when a non-diabetic’s blood glucose rises above 180 mg/dL during acute illness or injury, often confirmed by repeated testing.
Can stress-induced hyperglycemia lead to diabetes?
Yes, some people who experience stress-induced hyperglycemia may develop type 2 diabetes within a year, especially if risk factors are present.
What are the symptoms of stress-induced hyperglycemia?
Symptoms include frequent urination, excessive thirst, fatigue, blurred vision, and sometimes confusion or slow wound healing.
How is stress-induced hyperglycemia treated?
Treatment focuses on managing the underlying stressor, monitoring glucose, and sometimes using insulin in the hospital setting.