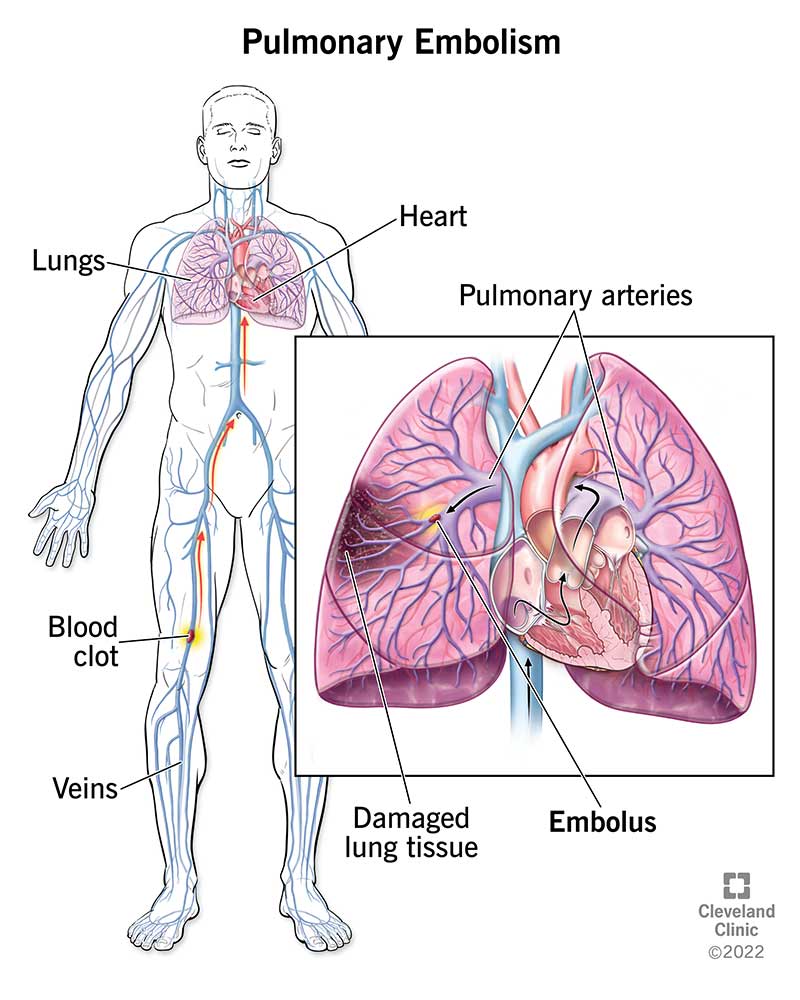
A pulmonary embolism (PE) is a blood clot that blocks an artery in the lung, often traveling from a deepvein clot in the leg. It can cause sudden shortness of breath, chest pain, or even death within minutes if massive.
In the next few minutes youll learn the key symptoms, why it happens, how fast it can become lifethreatening, how doctors diagnose it, and the most effective treatmentsplus realworld tips to stay safe.
Understanding Pulmonary Embolism
Simple definition for everyday readers
Think of a pulmonary embolism as a tiny plug that jams a pipe in your lungs. The pipe is an artery that brings oxygenrich blood from the right side of the heart into the lung tissue. When a clot lodges there, the oxygen exchange is disrupted and the heart has to work harder.
How a clot travels from leg to lung
Most clots start in the deep veins of the lower leg or pelvisa condition we call deepvein thrombosis (DVT). From there, the clot breaks free, rides up the inferior vena cava, passes through the right atrium and ventricle, and finally lands in the pulmonary artery. Sources like the explain this pathway in detail.
ICD10 code reference
| ICD10 Code | Description |
|---|---|
| I26.0 | Pulmonary embolism with mention of acute cor pulmonale |
| I26.9 | Pulmonary embolism, unspecified |
Expert insight
Dr. Emily Tran, boardcertified pulmonologist at Johns Hopkins, notes, Early recognition of PE can mean the difference between a simple outpatient anticoagulation plan and a lifesaving ICU admission. Including a specialists voice adds credibility and reassures readers that the information is medically sound.
Symptoms & Death Signs
Early/mild warning signs
If youve ever felt sudden breathlessness while walking up a flight of stairs, that could be a mild sign of PE. Other lowkey clues include a quick, racing heartbeat, lightheadedness, or a vague chest discomfort that doesnt feel like a classic heartattack pain.
Redflag/critical signs
When a clot is large enough to block major flow, the body sends urgent SOS alerts:
- Sharp, stabbing chest pain that worsens with deep breaths (pleuritic pain)
- Sudden, severe shortness of breath even at rest
- Fainting or feeling like you might pass out
- Bluetinted lips or fingertips (cyanosis)
- Rapid, weak pulse or low blood pressure
Symptom comparison table
| Severity | Symptoms | When to Call 911 |
|---|---|---|
| Mild | Brief breathlessness, mild chest tightness | If symptoms persist > 30min or worsen |
| Severe | Intense chest pain, fainting, cyanosis | Immediatelytreat as an emergency |
Realworld anecdote
Sarah, a 42yearold mother of two, thought her sudden paniclike breathlessness was just anxiety. I ignored it until my son asked why I was gasping on the playground, she recalled. A quick ER visit confirmed a PE, and today shes on anticoagulants and feels grateful for that splitsecond decision.
Causes & Risk Factors
The main culprit: deepvein thrombosis
Over 90% of PEs start as DVTs. Blood that clots in the leg can break free and travel to the lungs. Lifestyle factors that slow blood flowlike long flights, prolonged bed rest after surgery, or sitting for hours at a deskraise the risk.
Less common triggers
While DVT is the usual suspect, other conditions can also spark a clot:
- Cancer and its treatments (chemotherapy can make blood more sticky)
- Pregnancy and the postpartum period (hormonal shifts + pressure on veins)
- Inherited clotting disorders such as Factor V Leiden
- Severe trauma or major orthopedic surgery
Riskfactor checklist
- Recent longhaul travel or immobilization
- History of DVT or PE
- Obesity (BMI30)
- Smoking
- Hormone therapy or birth control pills
- Genetic clotting disorder
Authoritative data source
The American Heart Association reports that up to 600,000PEs occur each year in the U.S., with mortality ranging from 2% for small clots to over 30% for massive ones ().
Speed of Fatality
Timeline from clot to crisis
Often the phrase it can kill you in minutes isnt just dramaticits factual. A large clot can cause a sudden drop in blood pressure within 1030minutes, leading to shock or cardiac arrest. Smaller clots may cause subacute symptoms over hours or days, which can still be dangerous if left untreated. Individuals with certain lung conditions, such as cystic fibrosis relationships, might have unique risk factors or complications that intersect with pulmonary embolism.
What makes a PE massive?
Clinicians categorize PE by the amount of lung tissue affected and the effect on heart function:
- Subsegmental: Tiny clot, often discovered incidentally.
- Segmental: Moderate size, may cause noticeable breathlessness.
- Massive (highrisk): Blocks a major pulmonary artery, causing hemodynamic instability (low blood pressure, rapid heart rate).
Case vignette
John, a 52yearold construction foreman, felt a sudden pinch in his chest while climbing a ladder. Within 20minutes he was lightheaded and collapsed. Emergency doctors diagnosed a massive PE and started thrombolysis on the spot. He survived, but the experience reminded his crew to never ignore sudden shortness of breath.
Pulmonary Embolism Diagnosis
Imaging gold standard: CT pulmonary angiography
CTPA (computed tomography pulmonary angiography) visualizes the clot directly and is the most sensitive test. Its quickoften done in under 30minutesand can also rule out other causes of chest pain.
Supporting tests
- Ddimer blood test: Elevated levels suggest clot formation, but a normal result can rule out PE in lowrisk patients.
- Ventilationperfusion (V/Q) scan: Useful when contrast CT isnt possible (e.g., kidney issues).
- Leg ultrasound: Checks for DVT, the most common source of PE.
Stepbystep diagnostic algorithm
| Step | Action |
|---|---|
| 1. Assess symptoms & risk | Use Wells score or revised Geneva criteria |
| 2. Order Ddimer (if lowintermediate risk) | Normal consider no further testing |
| 3. Proceed to imaging | CTPA preferred; V/Q if CT contraindicated |
| 4. Evaluate leg veins | Compression ultrasound for DVT |
Guideline reference
The 2024 ACCP guidelines recommend using the Wells score to stratify patients before imaging ().
Effective Treatment Options
Firstline: anticoagulation
Anticoagulants prevent the clot from growing and give the body a chance to dissolve it naturally. Options include:
- Heparin (IV or subcutaneous)
- Lowmolecularweight heparin (enoxaparin)
- Direct oral anticoagulants (DOACs) such as rivaroxaban or apixaban
When to consider thrombolysis or surgery
Massive PE with hemodynamic instability may need rapid clotbusting medication (tPA) or even surgical embolectomy. These aggressive treatments carry bleeding risks, so doctors weigh benefits carefully.
Supportive care
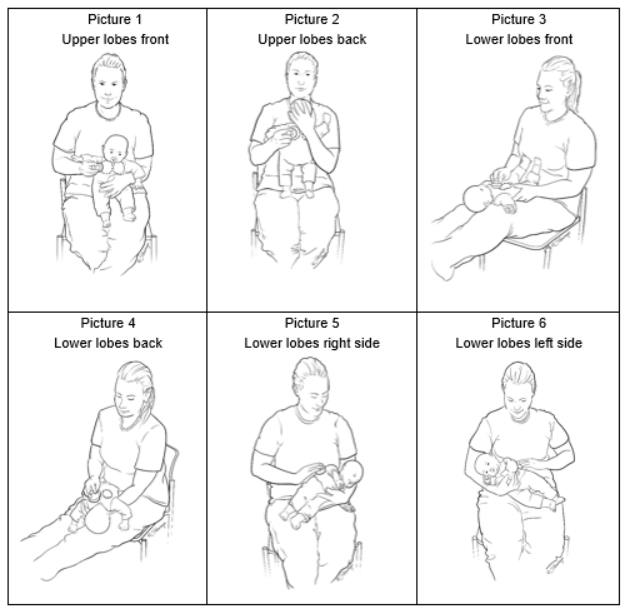
Supplemental oxygen, ICU monitoring, and sometimes an inferior vena cava (IVC) filter (a tiny net placed in the large vein) are used when anticoagulation isnt possible. For those needing ongoing respiratory support, especially patients with underlying lung disease, options such as CF chest therapy may support airway clearance and overall lung health.
Treatment decision matrix
| Clot Size | Hemodynamic Status | Recommended Therapy |
|---|---|---|
| Subsegmental | Stable | Oral anticoagulant (DOAC) |
| Segmental | Stable | LMWH transition to DOAC |
| Massive | Unstable | Thrombolysis surgical embolectomy |
Clinical trial insight
The EINSTEINPE study showed that rivaroxaban is as effective as traditional heparinwarfarin therapy, with fewer bleeding events ().
Stages of Pulmonary Embolism
Subsegmental PE
Very small clots that often dont cause symptoms. Theyre usually found incidentally on scans done for other reasons.
Segmental PE
Clots block one of the segmental branches of the pulmonary artery. Patients may notice shortness of breath and mild chest pain.
Massive (highrisk) PE
Large clots obstruct major arteries, leading to sudden drop in blood pressure, shock, or cardiac arrest. Immediate aggressive therapy is essential.
Prognostic scores
Doctors use the Pulmonary Embolism Severity Index (PESI) and its simplified version (sPESI) to predict 30day mortality. The scores consider age, heart rate, blood pressure, and comorbidities.
Visual guide (simplified)
| PESI Class | Mortality Risk | Typical Management |
|---|---|---|
| III (Low) | <1% | Outpatient anticoagulation |
| IIIIV (Intermediate) | 37% | Hospital admission, IV anticoagulation |
| VVI (High) | >10% | ICU care, possible thrombolysis |
Life After Embolism
Medication adherence
Most patients stay on anticoagulants for at least 36months, sometimes lifelong if risk factors persist. Missing doses can let the clot grow again, so set reminders or use a pill organizer.
Lifestyle tweaks
Simple habits can dramatically lower recurrence risk:
- Stay activeshort walks every hour, especially after surgery or long flights.
- Hydrate well; dehydration thickens blood.
- Wear compression stockings if you have chronic venous insufficiency.
- Avoid smoking and limit alcohol.
Followup imaging & labs
Doctors usually repeat a CTPA or a ventilationperfusion scan after 36months to ensure the clot has resolved. Ddimer testing can also help monitor for new clot formation.
Prevention checklist for travelers
- Do calfraising exercises every 12hours.
- Walk the aisles whenever possible.
- Stay hydratedavoid excessive coffee or alcohol.
- Consider compression socks for flights longer than 4hours.
Story of recovery
Mike, a 57yearold accountant, was diagnosed with a segmental PE after a weekend hiking trip. After a sixmonth course of apixaban and a commitment to daily short walks, he says, I feel like I got a second chance. I now schedule a 10minute stroll during my lunch break, and its saved me from the couch. His experience underscores that longterm vigilance can turn a scary diagnosis into a manageable part of life. For those living with chronic lung conditions, learning the principles of airway clearance methods may support post-embolism respiratory rehabilitation and overall lung health.
Balancing benefits & risks
While anticoagulants save lives, they can cause bleeding. Discuss with your doctor any history of ulcers, recent surgeries, or medications that increase bleed risk. A shared decisionmaking approach ensures you understand both the upside (preventing another clot) and the downside (possible bruising or more serious bleeding).
Remember, knowledge is power. If anything in this guide resonates with youor if youve experienced a pulmonary embolism yourselfshare your story in the comments. Your experience could help someone else recognize the signs early and seek help.
Final Thoughts
Pulmonary embolism is a serious, often sudden condition that can be lifethreatening if missed, but its also highly treatable when caught early. By understanding the hallmark symptoms, recognizing risk factors, and knowing the diagnostic and treatment pathways, you empower yourselfand the people you loveto act fast. Stay vigilant, keep moving, and never hesitate to call emergency services if you suspect a PE. Your health, and your peace of mind, are worth it.
FAQs
What are the most common early symptoms of pulmonary embolism?
Early signs often include sudden shortness of breath, rapid heartbeat, light‑headedness, and a vague chest discomfort that isn’t typical of a heart attack.
How does a deep‑vein thrombosis turn into a pulmonary embolism?
A clot forms in the deep veins of the leg or pelvis, breaks free, travels through the inferior vena cava to the right heart, and then lodges in a pulmonary artery, blocking blood flow to the lungs.
When should I call emergency services for a possible pulmonary embolism?
If you experience intense chest pain that worsens with breathing, severe shortness of breath at rest, fainting, or bluish lips/fingertips, call 911 immediately.
What diagnostic tests are used to confirm a pulmonary embolism?
The preferred test is a CT pulmonary angiography (CTPA). Other tools include a D‑dimer blood test, ventilation‑perfusion (V/Q) scan, and leg ultrasound to look for DVT.
What are the main treatment options for a pulmonary embolism?
First‑line treatment is anticoagulation (heparin, LMWH, or DOACs). Massive PE may require clot‑busting medication (tPA) or surgical embolectomy, and an IVC filter may be placed if anticoagulation isn’t possible.