Think of this as a coffeechat with someone whos done the homework, spoken to oncologists, and read the latest trial results. By the end, youll have a clear picture of the drug landscape, the standard soft tissue sarcoma chemotherapy protocol, the newest targeted agents, and practical tips for staying on top of sideeffects. Lets dive in, shall we?
Why It Matters
Knowing the drug landscape isnt just academicit directly impacts the chances of shrinking a tumor, preserving function, and maintaining quality of life. Sarcomas are a mixed bag; a drug that kills one subtype might do nothing for another. Thats why clinicians lean on soft tissue sarcoma treatment guidelines and why you, as a patient or caregiver, need to understand the why behind each choice.
Imagine youre at a bustling farmers market. Each stall sells different producesome apples, some exotic fruits. If you need a red fruit for a recipe, knowing which stall to visit saves you a lot of wandering. The same goes for sarcoma drugs: knowing which stall (drug class) matches your tumors genetics helps you avoid unnecessary trips (treatments) and get to the tasty fruit (response) faster.
Core Chemotherapy Drugs
Which agents are considered firstline?
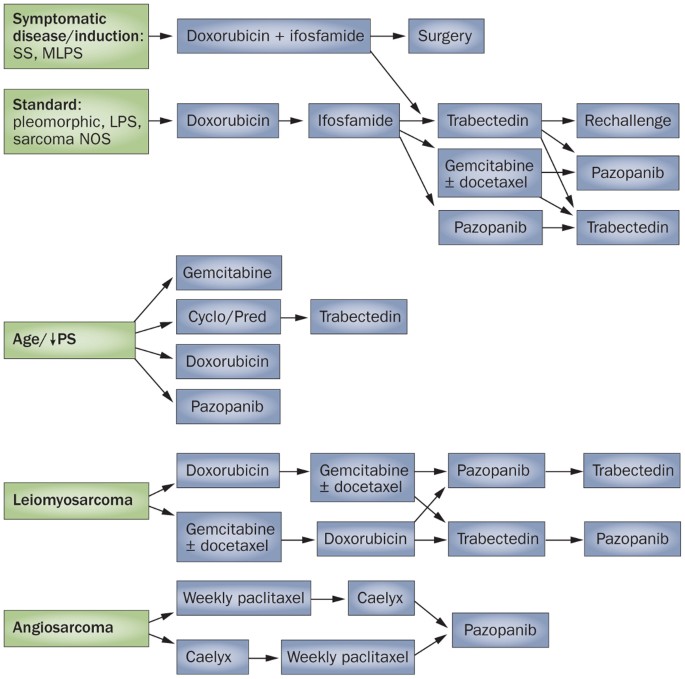
The backbone of most adult sarcoma regimens is still the classic duo of doxorubicin and ifosfamide. Add mesna to protect the bladder, and you have the most widely studied soft tissue sarcoma chemotherapy drugs. Other workhorses youll hear about include:
- Gemcitabine+Docetaxel often used when patients cant tolerate ifosfamide.
- Dactinomycin chiefly for pediatric cases but still appears in adult protocols for certain subtypes.
- Etoposide occasionally combined with ifosfamide in highrisk disease.
These drugs have been validated in dozens of trials and are referenced in the treatment summaries.
Standard dosing schedules and cycle length
Most regimens run in 21day cycles:
| Drug | Typical Dose (mg/m) | Cycle Length | Common Toxicities |
|---|---|---|---|
| Doxorubicin | 75 | Every 21 days | Cardiotoxicity, nausea |
| Ifosfamide + Mesna | 910 (ifosfamide) | Every 21 days | Neutropenia, cystitis |
| Gemcitabine | 1,000 | Days 1 & 8 of a 21day cycle | Thrombocytopenia, fatigue |
| Docetaxel | 75 | Same as gemcitabine | Hair loss, neuropathy |
These numbers are averagesyour oncologist will tailor them to your size, kidney function, and overall health. Speaking with a boardcertified sarcoma specialist can help you understand why a certain dose was chosen for you.
Standard Protocols
Classic doxorubicin+ifosfamide regimen
When the tumor is highgrade or unresectable, many teams start with three to six cycles of doxorubicin (75mg/m) followed by ifosfamide (910g/m total) given over three days, with mesna for bladder protection. The goal is to achieve a 50% shrinkage before surgery or radiation.
When is singleagent doxorubicin enough?
If youre older, have heart disease, or simply want to avoid the extra nausea of ifosfamide, doctors may opt for doxorubicin alone. While response rates dip a little (around 2025% versus 3035% with the combo), the tradeoff can be worth it for many patients.
Alternative protocols for ifosfamideintolerant patients
Some folks develop severe cystitis or kidney issues that make ifosfamide unsafe. In those cases, the gemcitabine+docetaxel pairing often steps in. Its a little gentler on the bladder and still gives respectable response rates, especially in leiomyosarcoma and undifferentiated pleomorphic sarcoma.
Realworld vignette
Take Maya, a 45yearold teacher whose thigh sarcoma refused to shrink after two cycles of doxorubicin alone. Her oncologist added ifosfamide, and by the end of cycle four, imaging showed a 55% reductionjust enough to allow a limbsparing surgery. Mayas story underscores how flexible protocols can adapt to the tumors behavior and the patients tolerance.
New Targeted Therapies
Approved agents for specific subtypes
Not all sarcomas are created equal. Some have a genetic Achilles heel that a targeted drug can exploit:
- Imatinib for dermatofibrosarcoma protuberans (DFSP) with the COL1A1PDGFB fusion.
- Pazopanib for unresectable, metastatic nonliposomal softtissue sarcomaworks as a multikinase inhibitor.
- Lorlatinib and Larotrectinib for NTRKfusion sarcomas, regardless of the anatomic site.
The maintains an uptodate list of these subtypespecific drugs.
Latestage trials and new sarcoma cancer drug candidates
Several promising agents are in phaseIII studies as of 20242025:
- Vimseltinib a novel CSF1R inhibitor showing activity in undifferentiated sarcoma.
- Tazemetostat an EZH2 inhibitor useful for INI1deficient tumors.
- Selinexor a selective exportin1 inhibitor that may overcome resistance to standard chemo.
These trials often allow patients to enroll through academic centers, offering a chance to receive cuttingedge therapy before it hits the market. If youre interested, ask your oncologist about current options.
Sidebyside comparison
| Drug | Approved Indication | Mechanism | PhaseIII ORR | Approval Year |
|---|---|---|---|---|
| Imatinib | DFSP (COL1A1PDGFB) | TKI (PDGFR) | ~70% | 2006 |
| Pazopanib | Metastatic nonliposomal STS | Multikinase | ~12% | 2012 |
| Larotrectinib | NTRKfusion sarcomas | TRK inhibitor | ~75% | 2020 |
Managing Side Effects
Top three toxicities with doxorubicin & ifosfamide
1. Cardiotoxicity Doxorubicin can strain the heart, especially after a cumulative dose >450mg/m. Baseline echo and periodic monitoring are essential.
2. Neutropenia Both drugs suppress bone marrow. Growthfactor support (GCSF) may be prescribed to keep infections at bay.
3. Bladder irritation (hemorrhagic cystitis) Ifosfamides metabolite acrolein hurts the bladder lining. Thats why mesna is nonnegotiable and aggressive hydration is advised.
Mitigating nausea, fatigue, and other everyday woes
- Antiemetics*: ondansetron, dexamethasone, or newer NK1 antagonists.
- Hydration*: sip a water bottle every 30minutes during infusion days.
- Nutrition*: small, frequent meals with bland foods; consider ginger tea for nausea.
- Activity*: gentle walks or stretching to combat fatigue, but listen to your body.
Supportivecare checklist
- Baseline blood work (CBC, CMP) and cardiac echo.
- Mesna schedule aligned with ifosfamide infusion.
- Plan for GCSF on day56 if neutrophils dip.
- Symptomtracking app (many patients love Cancer.Net Mobile).
Balancing benefits and risks is a core part of the conversation. No one wants to feel like theyre choosing death versus choosing sideeffects, but understanding the tradeoffs lets you and your doctor make an informed, shared decision.
RealWorld Decisions
Chemo for sarcoma in lungs versus other sites
When sarcoma spreads to the lungs, the disease behaves a bit differently. Systemic chemo still reaches the lungs, but some clinicians add local therapies (e.g., stereotactic body radiation). Studies show that soft tissue sarcoma chemotherapy drugs can shrink pulmonary nodules in ~30% of cases, buying time for surgery or ablative procedures.
Patient preferences, comorbidities, and qualityoflife scores
Imagine youre juggling a fulltime job, a toddler, and a heart condition. You might prioritize a regimen with fewer hospital days, even if the response rate is a shade lower. Tools like the EORTC QLQC30 questionnaire help capture your values, and most oncologists welcome that data when shaping the plan.
Clinical trials: when theyre the best option
Clinical trials arent a lastditch effort; theyre often the fastest route to the newest, most effective drugs. If youre under 65, have good organ function, and can commit to extra visits, a trial might let you access a new sarcoma cancer drug before its FDAapproved. Ask your care team about open studiessometimes a quick phone call can open a door.
ProsCons table for major regimens
| Regimen | Pros | Cons |
|---|---|---|
| Doxorubicin+Ifosfamide | High response rates; wellstudied | Cardiotoxicity, bladder irritation, more nausea |
| Gemcitabine+Docetaxel | Less cardiac risk; good for ifosfamideintolerant pts | Lower overall response; fatigue |
| Pazopanib (singleagent) | Oral administration; tolerable for many | Modest response; liver enzyme monitoring needed |
| Clinical trial (e.g., Vimseltinib) | Access to cuttingedge therapy; potential for high response | Uncertain longterm safety; more frequent visits |
Quick Answers to Common Questions
Can softtissue sarcoma be treated with oral pills alone? For a few subtypes (like DFSP with imatinib), yes. Most highgrade sarcomas, however, still need IV chemotherapy to reach a therapeutic level.
Is fenbendazole a legitimate option? The antiparasitic drug has no convincing clinical evidence for sarcoma. Reputable sources (e.g., the ) warn against unproven miracle cures. Stick to therapies backed by trials.
What do sarcoma images of the legs look like? Classic CT or MRI scans show a heterogeneous mass often infiltrating muscle layers. If youre curious, the NCIs image gallery offers soft tissue sarcoma pictures legs that illustrate typical appearances.
Conclusion
Navigating the world of soft tissue sarcoma drugs can feel overwhelming, but you dont have to do it alone. The core chemotherapy agentsdoxorubicin, ifosfamide, gemcitabine, and docetaxelremain the workhorses, while newer targeted therapies like pazopanib and larotrectinib hand out precisionmedicine treats to specific subtypes. Understanding the standard soft tissue sarcoma chemotherapy protocol, the likely sideeffects, and where clinical trials might fit into your journey equips you to ask the right questions and partner with your oncologist effectively.
Remember, each persons story is unique. If something feels off, speak up. If you have a question about a particular drug, a sideeffect youre experiencing, or a trial you heard about, drop a comment below or reach out to a trusted cancercare professional. Were all in this together, and the more we share, the stronger our community becomes.
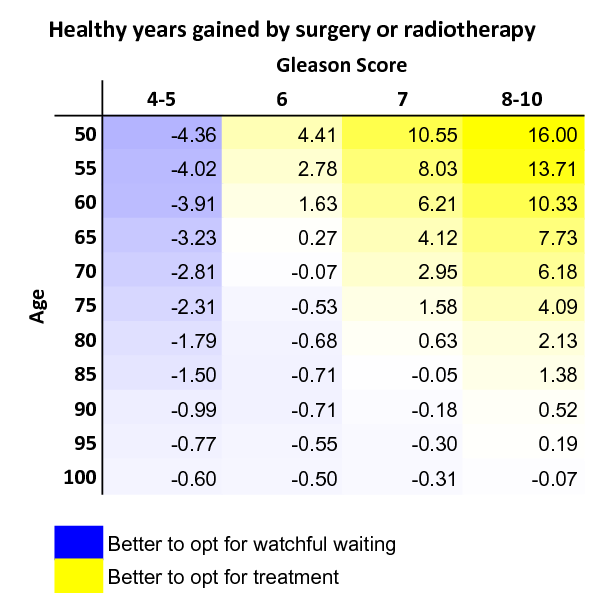
For readers also managing prostate concerns or researching longterm outcomes, consider this overview on prostate cancer outlook which discusses survival trends and factors that influence life expectancy after prostate treatments.
FAQs
What is the standard first‑line chemotherapy for soft tissue sarcoma?
The most common initial regimen combines doxorubicin (75 mg/m²) with ifosfamide (9–10 g/m² total) given every 21 days, often with mesna to protect the bladder.
Are there any effective oral drugs for soft tissue sarcoma?
Yes. Pazopanib is an FDA‑approved oral multi‑kinase inhibitor for metastatic non‑liposomal sarcoma, and several targeted agents (e.g., imatinib for DFSP, larotrectinib for NTRK‑fusion sarcoma) are also taken by mouth.
How is the risk of heart damage from doxorubicin managed?
Cardiotoxicity is monitored with baseline and periodic echocardiograms or MUGA scans. The cumulative dose is usually kept below 450 mg/m², and dose reductions are made if heart function declines.
When should a patient consider enrolling in a clinical trial?
Clinical trials are often recommended when the disease progresses after standard therapy, when a specific genetic alteration matches an investigational drug, or when a patient seeks access to cutting‑edge treatments not yet approved.
Which sarcoma subtypes have dedicated targeted therapies?
Examples include imatinib for dermatofibrosarcoma protuberans (COL1A1‑PDGFB fusion), larotrectinib or entrectinib for NTRK‑fusion sarcomas, and tazemetostat for INI1‑deficient tumors.