Think of a childs blood as the delivery truck that brings oxygen to every corner of the body. When that truck is shortchanged, youll notice the little engine sputteringtiredness, pale skin, slower growth. Thats pediatric anemia in a nutshell.
In the next few minutes youll discover what pediatric anemia really means, why it shows up, how doctors pinpoint it (yes, there are ), and the safest ways to treat and prevent it. Ready? Lets dive in together.
What Is Pediatric Anemia?
Definition & How It Differs From Adult Anemia
Simply put, pediatric anemia is a condition where a childs redbloodcell countor the amount of hemoglobin inside those cellsis below the ageadjusted normal range. Adults and kids arent measured the same way; a hemoglobin level thats fine for a teenager might signal trouble for a toddler.
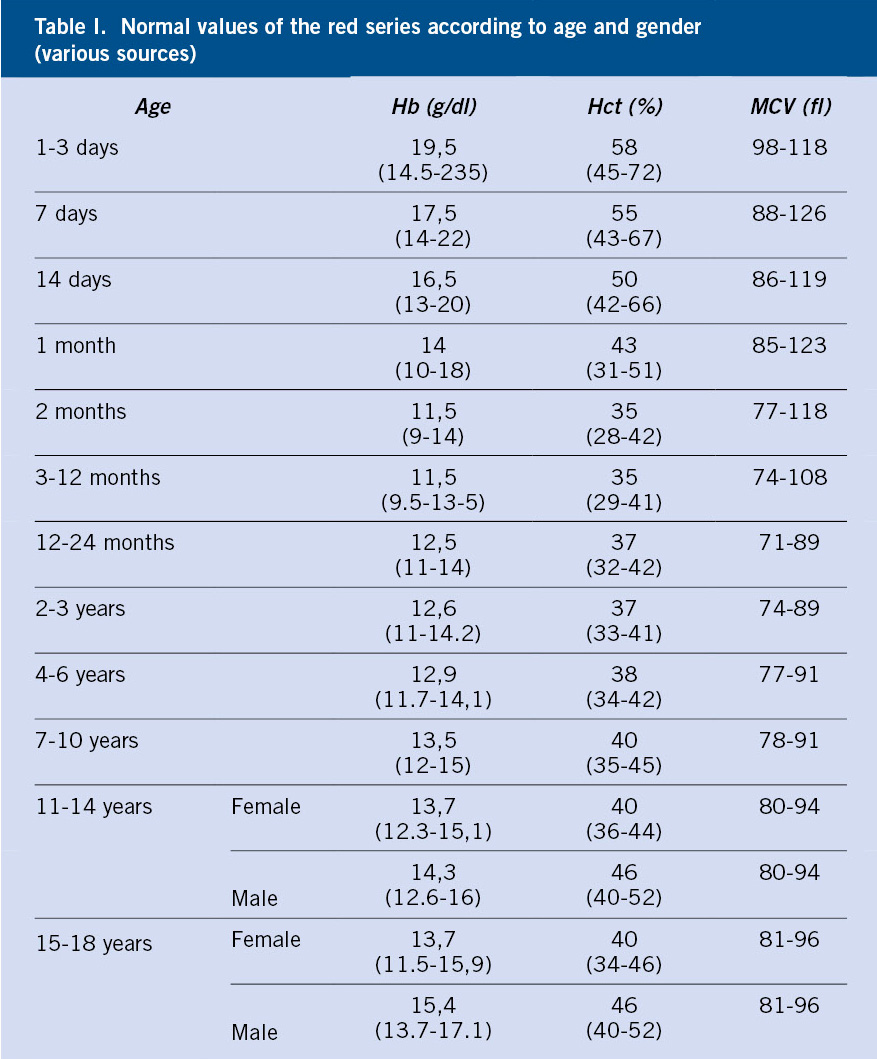
Normal Hemoglobin Ranges by Age
| Age | Typical Hemoglobin (g/dL) |
|---|---|
| Newborn (02weeks) | 13.520.0 |
| Infant (212months) | 10.513.0 |
| Toddler (13years) | 11.013.0 |
| Preschool (45years) | 11.513.5 |
| Schoolage (612years) | 12.015.5 |
| Adolescent (1318years) | 12.016.0 |
Why the Numbers Matter
When hemoglobin dips below these thresholds, the bodys oxygencarrying capacity drops. The result? Fatigue, pallor, and if untreated, delayed growth or developmental setbacks. Knowing the numbers helps parents and clinicians catch the problem early.
Common Types of Anemia
IronDeficiency Anemia
By far the most frequent culprit. Kids who are picky eaters, drink excessive cows milk, or have rapid growth spurts can outgrow their iron stores fast.
Vitamin B12 / Folate Deficiency
Less common, but still importantespecially in children with restrictive diets (think vegan families) or malabsorption issues.
Hemolytic Anemia (SickleCell & Thalassemia)
These are genetic conditions where red cells break down prematurely. Theyre more prevalent in certain ethnic groups, and they often require specialist care.
Anemia of Chronic Disease
Longstanding illnesseslike kidney disease, inflammatory bowel disease, or recurrent infectionscan tug at the marrows ability to produce enough healthy cells.
Quick Comparison
| Type | Key Cause | Lab Clues | Typical Age |
|---|---|---|---|
| IronDeficiency | Inadequate intake or loss | Low ferritin, high TIBC | 6months5years |
| B12/Folate | Dietary deficiency, malabsorption | High MCV, low B12/folate | 212years |
| Hemolytic | Genetic RBC disorder | Elevated LDH, low haptoglobin | Birthteen |
| Chronic Disease | Underlying illness | Normal/high ferritin, low iron | Any age |
Why Children Develop Anemia
Inadequate Dietary Iron or Vitamins
Think of iron as the fuel for the redcell engine. When kids swap spinach for cheese sticks, that engine sputters. A diet low in ironrich foods (red meat, lentils, fortified cereals) is a leading cause.
Rapid Growth Periods
From 624months and again at early school age, children grow like weeds. Their blood has to keep up, and sometimes it cant, especially if iron stores were already thin.
Blood Loss
Subtle lossestiny gut bleeds from a worm infection, heavy menstrual periods for adolescent girls, or even frequent nosebleedscan add up and tip the balance.
Genetic Disorders
Sicklecell disease, thalassemia, and hereditary spherocytosis are inherited engine faults. Theyre not preventable, but early detection helps manage impacts.
Chronic Illnesses
Kidney disease, inflammatory bowel disease, or longstanding infections keep the body in a stress mode, diverting iron away from redcell production.
5 Common Culprits at a Glance
- Poor iron intake
- Fast growth spurts
- Hidden blood loss
- Inherited redcell disorders
- Chronic medical conditions
Spotting Symptoms Early
Classic Signs
Look for paleness (especially on the inside of the lower eyelids), unusual fatigue, rapid heartbeat, shortness of breath after mild activity, or frequent dizziness.
Subtle Clues
Sometimes the warning lights are dimmer: irritability, trouble concentrating at school, or growth that seems slower than classmates.
When Symptoms Mimic Other Issues
Asthma, heart problems, or even a cold can masquerade as anemia. Thats why a simple blood test is the gold standard for confirmation.
Checklist for Parents
Download a printable and tick off any that sound familiar. Its a quick way to decide whether a doctors visit is warranted.
How Doctors Diagnose
FirstLine Labs
A complete blood count (CBC) reveals hemoglobin level, hematocrit, and redcell size. If irondeficiency is suspected, ferritin, serum iron, and total ironbinding capacity (TIBC) follow.
When to Order a Peripheral Smear or Electrophoresis
If the CBC hints at abnormal cell shapes or sizes, a blood smear can spot sickle cells or fragmented red cells. Hemoglobin electrophoresis is the goto test for sicklecell disease and thalassemia.
Guidelines That Guide the Process
The current from the American Academy of Pediatrics recommend screening at 912months, again at 2430months, and before school entry. Following these checkpoints catches most cases before symptoms become severe.
From Visit to Diagnosis
- Wellchild check CBC ordered
- Lab returns: low hemoglobin? iron studies
- If iron studies normal consider genetic or chronicdisease workup
- Confirm with specialized tests (electrophoresis, bonemarrow aspirate) as needed
Treatment Options Overview
Iron Supplementation
Oral ferrous sulfate is the usual first steptypically 3mg/kg of elemental iron per day, divided into two doses. Common side effects include stomach upset and dark stools; taking the supplement with food (but not dairy) can ease discomfort.
Vitamin B12 / Folate Replacement
For deficiency, injectable B12 or highdose oral tablets are effective. Folate (folic acid) is usually given as 0.5mg daily for a few weeks, then tapered.
When Transfusion Is Needed
Severe anemia (hemoglobin <7g/dL) or symptomatic children with rapid heart rates may require a packed redcell transfusionalways a shortterm bridge while the underlying cause is treated.
Managing Chronic or Hemolytic Anemias
Therapies vary: hydroxyurea is a mainstay for sicklecell disease; iron chelation helps when repeated transfusions cause iron overload; newer geneediting trials are offering hope for future cures.
Medication vs. Age Safe Dosing Guidelines
| Medication | Age Range | Typical Dose |
|---|---|---|
| Ferrous Sulfate | 6months12years | 3mg/kg elemental iron/day |
| Vitamin B12 (Cyanocobalamin) | All ages | 1mg IM weekly (initial), then monthly |
| Hydroxyurea | 5years18years (sicklecell) | 1535mg/kg/day |
Prevention & Lifestyle Tips
IronRich Foods for Every Age
Infants (612months): ironfortified cereals, pureed meats, and lentils. Toddlers: softcooked beans, chopped spinach, and lean beef strips. Schoolage kids: turkey, tofu, quinoa, and wholegrain breads.
VitaminC Pairing
VitaminC boosts iron absorption. A squeeze of orange juice over oatmeal or a side of strawberries with a bean salad can make a noticeable difference.
Safe Supplementation
Dont give iron tablets to a child who isnt irondeficientoverdose can be toxic. Always follow the pediatricians dosing instructions.
Routine Screening Schedule
The AAP recommends a CBC check at 912months, again at 2430months, and a final screen before kindergarten. If your child has risk factors (premature birth, chronic illness, exclusive breastfeeding beyond 6months without ironfortified formula), discuss earlier testing with your doctor.
PrintReady Screening Schedule
Grab the free and keep it on your fridge. A quick glance each year helps you stay on track.
Quick Resources & Tools
Downloadable PDFs
- Pediatric Anemia Guidelines PDF comprehensive recommendations from the AAP.
- Symptoms Checklist a onepage tool for busy parents.
- Screening Schedule reminders for each developmental milestone.
Interactive HemoglobinAge Calculator
Enter your childs age and hemoglobin result to see instantly whether the level falls within the normal range. (Embed widget placeholder)
Further Reading
For deeper dives, see the and the latest review in Pediatrics on anemia management in children.
Conclusion
Pediatric anemia is more common than many realize, but its also highly treatable when caught early. By recognizing the telltale signs, understanding the underlying causes, and following trusted pediatric anemia guidelines, you can ensure your child gets the right carefast. Download the free tools, talk openly with your pediatrician, and remember youre not alone; experts and countless families have walked this path and emerged healthier together.
FAQs
What are the most common signs of pediatric anemia?
Typical signs include pale skin (especially inside the lower eyelids), fatigue, rapid heartbeat, shortness of breath after mild activity, and irritability.
How is pediatric anemia diagnosed by doctors?
Doctors start with a complete blood count (CBC) to check hemoglobin levels. If low, they order iron studies, a peripheral smear, or hemoglobin electrophoresis based on the suspected type.
When should a child with anemia receive an iron supplement?
Oral iron is recommended when blood tests show iron‑deficiency anemia, usually at a dose of 3 mg/kg elemental iron per day divided into two doses, unless contraindicated.
Can diet alone prevent pediatric anemia?
Providing iron‑rich foods such as fortified cereals, lean meats, beans, and pairing them with vitamin C sources helps, but children at risk may still need a pediatrician‑prescribed supplement.
What are the treatment options for severe anemia in children?
Severe cases (hemoglobin < 7 g/dL) may require a packed red‑cell transfusion while the underlying cause—iron deficiency, vitamin deficiencies, or chronic disease—is being addressed.