Bottom line: hip pain, a limp, or reduced motion in a growing youngster should set off an alarm bell. Prompt diagnosis and the right treatment can keep the hip healthy and sidestep painful longterm issues. Lets dive into what it is, why it happens, and how to handle itwithout the jargon overload.
Understanding the Slip
What Exactly Is a Femoral Head Slip?
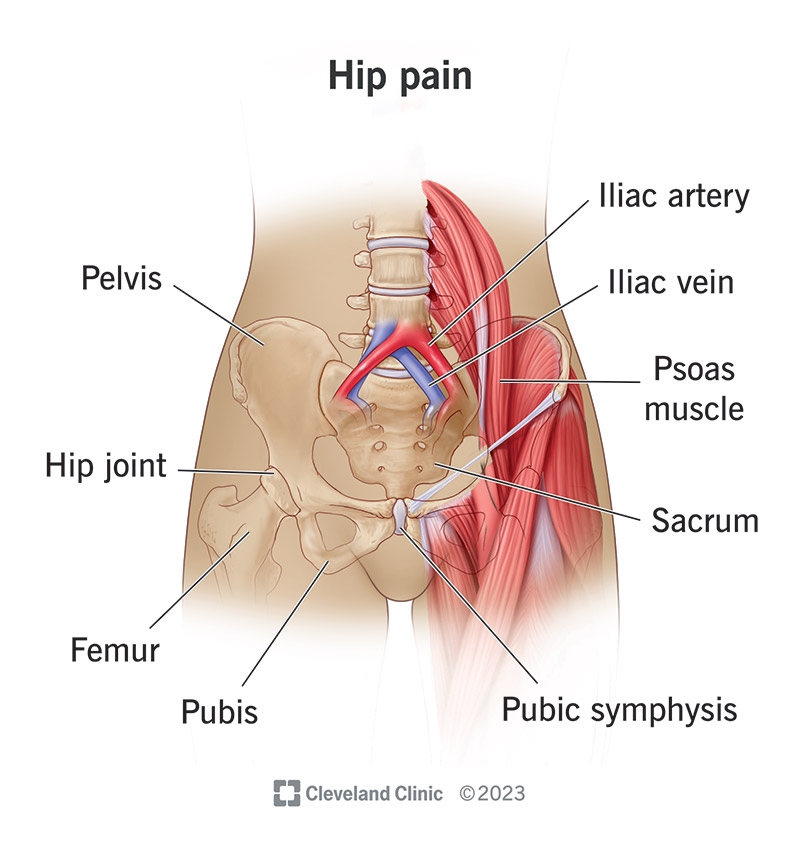
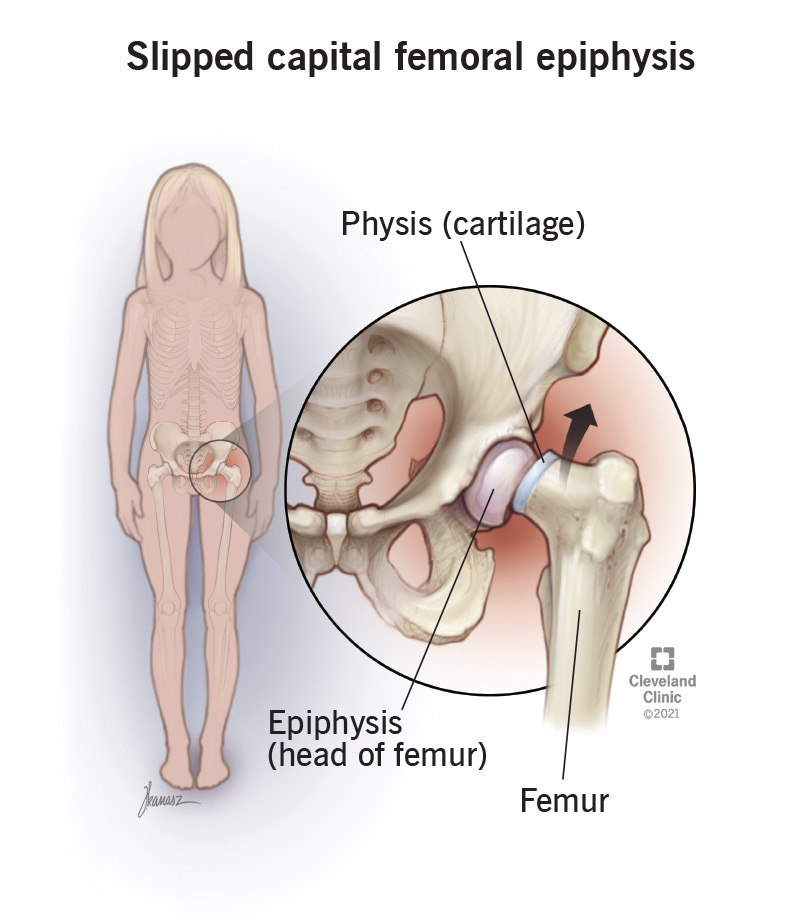
The femur (thigh bone) ends in a round ball called the femoral head. In children and adolescents, this ball is attached to the neck of the bone by a soft, cartilaginous growth plate (the physis). In SCFE, that growth plate weakens and the ball slides off the neckusually backward and downward. Think of it like the tip of an icecream cone slipping off the cones side while youre trying to eat it.
How Common Is It?
SCFE is one of the most frequent hip disorders affecting growing kids, especially in the United States and Europe. Roughly 1 in 10,000 children will develop it each year, according to the American Academy of Orthopaedic Surgeons ().
Why Use Femoral Head Slip Instead of SCFE?
Most people search for femoral head slip because it sounds less technical. Using the main keyword helps the article show up right where youre looking. But dont worrywell keep the medical term SCFE handy for the deeper details.
Quick Fact Box
| Term | Synonyms | ICD10 Code |
|---|---|---|
| Femoral Head Slip | Slipped Capital Femoral Epiphysis (SCFE) | M92.41 |
Who Gets It?
Typical Age Range
Most slips happen between ages 1014 for girls and 1216 for boysright when kids are shooting up like rockets. Rapid growth, combined with a soft growth plate, creates the perfect storm.
Key Risk Factors
- Obesity: Extra weight puts more stress on the growth plate.
- Hormonal disorders: Conditions like hypothyroidism or growth hormone excess can weaken the physis.
- Genetics & ethnicity: Higher rates are seen in AfricanAmerican and Hispanic populations.
Can Adults Experience a Slip?
Its rare, but it does happen. Adult cases usually stem from an untreated adolescent slip or from secondary hip disease that compromises the joint. When it shows up in an adult, its often called a slipped hip joint in adults and can be trickier to treat.
Case Vignette
Emily, a 15yearold soccer player, felt a sudden catch in her right hip after a sprint. A quick Xray revealed a stable slip. Jake, 28, waited years after a mild childhood slip and now faces an unstable slip with joint degeneration. Their stories show why early detection matters.
Spotting the Slip
Classic Symptoms
Kids with a femoral head slip often describe a vague ache in the groin or outer thigh, especially after activity. They may limp, and their range of motionespecially internal rotationgets limited. Some say it feels like the hip locked or caught.
Physical Exam Moves
Doctors perform a few key tests:
- Drehmann sign: The patients leg externally rotates as they try to flex the hipan almost textbook sign.
- Gait assessment: A limp that improves when the child stands on their toes can hint at SCFE.
ImagingHow Long Does SCFE Surgery Take?
The first step is a plain Xray (AP and frogleg lateral views). A classic picture shows the epiphysis shifted posteriorly and inferiorly. For borderline cases, an MRI can spot early slips before they become obvious on Xray. For families wanting clear, reliable guidance on diagnostic criteria and follow-up, refer to the ankylosing spondylitis criteria overview for an example of how clinical criteria are structured and applied in musculoskeletal conditions.
Image Comparison (text description)
Stable slip: The epiphysis is mildly displaced but remains attached.
Unstable slip: The ball is significantly displaced and risks blood supply loss.
Treatment Options
When Is NonSurgical Care Enough?
Very few stable slips respond to casting or activity restriction alone. Most orthopaedic surgeons recommend surgical fixation even for mild cases because it prevents further slippage and protects the blood supply.
Standard Surgical Fixation
The goto procedure is insitu pinning. A single cannulated screw is placed across the growth plate, locking the femoral head in its current position. Its quick, effective, and preserves most of the hips natural anatomy.
Advanced Techniques for Severe Cases
- Closed reduction & internal fixation (CRIF): Used for unstable slips where the bone needs to be gently repositioned before screwing it in.
- Modified Dunn procedure: A more complex reconstruction that realigns the head fully, reducing future arthritis risk but demanding a skilled surgeon.
Procedure Timeline
| Procedure | Typical Duration | Hospital Stay |
|---|---|---|
| Insitu pinning | 4590 minutes | 1 night |
| CRIF | 90120 minutes | 2 nights |
| Modified Dunn | 23 hours | 34 nights |
PostOp Care & Rehab
After surgery, most kids are nonweightbearing for 46 weeks. Physical therapy focuses on gentle rangeofmotion exercises, then gradual strengthening. Most return to sports within 46 months, but the timeline varies.
Parent Checklist
- Follow the surgeons weightbearing instructions to the letter.
- Watch for signs of infection: fever, increasing pain, or drainage.
- Keep followup Xrays on scheduleyour surgeon wants to see the screw staying put.
Long-Term Outlook
ShortTerm Risks
Even with prompt fixation, complications can arise:
- Avascular necrosis (AVN): Loss of blood to the femoral head, occurring in 510% of cases.
- Chondrolysis: Rapid cartilage loss, a rare but serious problem.
LongTerm Effects
Without proper treatment, SCFE can lead to early hip osteoarthritis, altered gait, and leglength discrepancy. A study in notes that up to 30% of patients develop arthritis by age 50.
Monitoring Into Adulthood
Regular orthopedic checkups every 12 years after the initial healing phase help catch any developing issues early. Staying active, maintaining a healthy weight, and avoiding highimpact sports before the hip fully matures are practical steps.
FollowUp Story
Laura, treated at age 13 with insitu pinning, attended yearly visits for five years. By age 22, her Xrays were clear, and shes now a marathon runnerproof that with the right care, a femoral head slip doesnt have to dictate your future.
Expert Insights
What Surgeons Say
Dr. Mark Jensen, a pediatric orthopedic specialist at Johns Hopkins, emphasizes, Early detection and timely stabilization are the keys to preserving hip health. The decision between a simple screw and a more involved reconstruction depends on the slips stability and the patients longterm activity goals.
Guidelines to Trust
The American Academy of Orthopaedic Surgeons clinical practice guideline recommends insitu pinning for most stable slips, reserving the modified Dunn for severe, unstable cases ().
Where to Find Help
If you suspect a femoral head slip, consider contacting a pediatric orthopedic centerplaces like , , or the orthopaedic department at your local university hospital. These institutions have surgeons who routinely perform SCFE surgery and can provide the multidisciplinary support you need.
Conclusion
Discovering a femoral head slip can feel overwhelming, but the good news is that its a treatable condition when caught early. Understanding the signs, knowing whos at risk, and acting quickly to get proper imaging and surgery can protect the hip and keep your childor even an adulton the path to an active, painfree life. Remember, youre not alone; experts, support groups, and reliable medical centers are ready to help you navigate every step. If youve experienced this or have questions, share your story below or reach out to a trusted pediatric orthopaedic specialist. Together, we can keep those hips moving smoothly for years to come.
FAQs
What are the early signs of a femoral head slip?
Kids often notice a vague groin or thigh ache, a limp that improves when walking on tip‑toes, and reduced internal rotation of the hip.
How is a femoral head slip diagnosed?
Plain X‑rays (AP and frog‑leg lateral views) reveal the displaced epiphysis; MRI is used for very early or subtle slips.
What are the treatment options for a stable slip?
Most surgeons perform in‑situ pinning with a single cannulated screw; this locks the femoral head in place while preserving growth.
What complications can arise after surgery for SCFE?
Potential issues include avascular necrosis, chondrolysis, screw migration, and later hip osteoarthritis.
How can I prevent a femoral head slip in my child?
Maintain a healthy weight, monitor rapid growth periods, and seek prompt evaluation for any unexplained hip pain or limp.