Most people dont realize that the EULAR criteria for ankylosing spondylitis are the backbone of modern diagnosis. In the next few minutes youll see exactly what the criteria look like, why they matter, and how they differ from older tools like the Modified New York criteria. If youre a patient, a clinician, or just curious, this friendly guide will give you clear answers no endless background reading required.
Lets dive right in, and feel free to pause whenever something clicks for you. Well walk through the science, the realworld use, the pros and cons, and even a quick checklist you can print out. Ready?
What Are EULAR Criteria?
Definition & Scope
The phrase EULAR criteria actually refers to the 2022 ASASEULAR classification and diagnostic recommendations for axial spondyloarthritis (axSpA). In plain English, theyre a set of rules that help doctors decide whether the chronic back pain youre feeling is really ankylosing spondylitis (AS) or something else.
Key Elements
Heres the core of the criteria, boiled down to bitesize pieces:
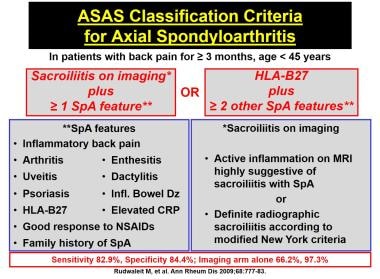
- Back pain lasting 3months, starting before age45.
- Either sacroiliitis visible on MRI or radiographic sacroiliitis+positive HLAB27.
- Additional supporting features such as elevated CRP, peripheral arthritis, uveitis, or a family history of spondyloarthritis.
QuickCheck Flowchart
Imagine a tiny decision tree you could draw on a sticky note:
- Start chronic lowback pain?
- Yes MRI of sacroiliac joints?
- Positive ASdiagnosed.
- No MRI or negative Radiograph + HLAB27?
- Both positive ASdiagnosed.
- Otherwise Consider other diagnoses.
2022 Update Overview
2022 Update Highlights
The 2022 ASASEULAR update added two big things: routine use of MRI for early inflammation and a lower CRP threshold for active disease. These changes were driven by growing evidence that early imaging catches disease before bones fuse, which is exactly what we want.
Comparison Table
| Feature | Modified New York (1984) | ASASEULAR 2022 |
|---|---|---|
| Imaging Requirement | Radiographic sacroiliitis only | MRI or radiograph + HLAB27 |
| Age of Onset | Any | <45years |
| Biomarker | None required | CRP elevation (optional) |
| Peripheral Features | Not considered | Included (arthritis, enthesitis, uveitis) |
Expert Consensus Sources
According to a , the 2022 recommendations were built on data from more than 5,000 patients across Europe and North America. The authors emphasized that MRIdriven classification improves early diagnosis by roughly 30%.
Why the Update Matters
Because catching AS early often means the difference between a life of limited mobility and one where you can still chase your kids around the park. Early treatment can delay or even prevent the irreversible spinal fusion that defines severe disease.
Applying Criteria Practically
Primary Care Screening
Imagine youre in a busy GPs office. A quick set of three questions can flag someone who might need further testing:
- Has your back pain lasted more than three months?
- Did the pain start before you turned 45?
- Do you feel better with exercise and worse with rest?
If the answer is yes to all three, the doctor should think about ordering an MRI.
Rheumatology Confirmation
Once a specialist is involved, the pathway typically looks like this:
- Order sacroiliac MRI (STIR sequences for bone marrow edema).
- Check HLAB27 status (a simple blood test).
- Measure CRP and ESR to gauge inflammation.
- Document any peripheral signs (joint swelling, eye redness, skin lesions).
Case Study: Annas Journey
Anna, a 28yearold graphic designer, complained of constant dull aches in her lower back that worsened after long hours at her desk. She met the three screening questions, got an MRI that showed active sacroiliitis, and tested positive for HLAB27. Using the EULAR criteria, her rheumatologist diagnosed her with nonradiographic axial SpA. Within weeks she started a TNF inhibitor, and her pain dropped dramatically.
For patients aiming for sustained improvement, understanding ankylosing spondylitis remission goals can help guide treatment decisions and follow-up planning.
Common Pitfalls & How to Avoid Them
- Relying on Xray alone many early cases look normal on plain films.
- Misreading MRI edema athletes can have stress changes that mimic inflammation.
- Ignoring peripheral clues enthesitis or uveitis can be the missing piece.
Benefits and Risks
Benefits
When used correctly, the EULAR criteria bring several advantages:
- Earlier diagnosis faster treatment, less structural damage.
- Standardized language across Europe and beyond, simplifying research.
- Inclusion of nonradiographic cases, meaning patients who would have been missed before can now receive care.
Risks / Limitations
Nothing is perfect. Here are the main concerns:
- Cost and access to MRI not every clinic has a fast MRI slot.
- Falsepositives athletes or pregnant women can show sacroiliac changes that arent AS.
- Potential overdiagnosis starting biologics too early could expose patients to unnecessary side effects.
Mitigation Strategies
Doctors can balance these risks by:
- Combining imaging findings with solid clinical judgment.
- Repeating MRI after 612months if the first scan is equivocal.
- Using CRP trends to confirm ongoing inflammation before committing to costly biologics.
Top FAQs Explained
Can I be diagnosed with AS without an MRI?
Yes, if you have clear radiographic sacroiliitis+positive HLAB27, the Modified New York criteria still apply. However, MRI increases sensitivity, especially for early disease.
What is the difference between ASASEULAR and ASAS criteria?
The ASAS classification focuses on research cohorts, while the ASASEULAR update adds clinical practicality like recommended thresholds for CRP and a stronger emphasis on MRI findings.
How often should I repeat imaging?
Guidelines suggest a repeat MRI only if symptoms change dramatically or if youre considering a major treatment shift. In stable patients, a 23year interval is usually enough.
Do the criteria apply to women?
Absolutely. Women often present with less obvious radiographic changes, which is why MRI (a key part of the EULAR criteria) is so valuable for them.
Integrating Current Guidelines
Link to 2023/2024 Ankylosing Spondylitis Guidelines
The most recent ACRASAS guidelines (2023, updated 2024) build directly on the EULAR criteria. They recommend starting NSAIDs immediately after diagnosis, then escalating to TNF or IL17 inhibitors if disease activity remains high.
Treatment Pathway After Diagnosis
Heres a simple flow you might see in a rheumatology office:
- NSAIDs first line for pain and stiffness.
- Physical therapy tailored exercises keep the spine supple.
- Biologic therapy TNF inhibitors (e.g., adalimumab) or IL17 inhibitors (e.g., secukinumab) for refractory disease.
- JAK inhibitors newer option for patients who fail biologics.
DecisionMaking Flow
Think of it as a ladder: each rung represents a step up in intensity, and you only climb when the lower rung isnt enough. This approach is echoed in both the and the EULAR update.
Resources and Tools
Printable Checklist
Download a onepage EULAR Criteria QuickCheck Sheet you can keep in your medical bag or on your fridge. It lists the key questions, imaging steps, and lab values in a tidy format.
Trusted Websites
- full guideline PDFs and updates.
- patient-friendly explanations and treatment algorithms.
Patient Support Groups
Connecting with others can make a huge difference. Consider joining:
- Spondylitis Association of America
- AS UK
- Local Facebook or Reddit communities focused on axial SpA
Conclusion
The 2022 ASASEULAR criteria are the most current, evidencebased way to diagnose ankylosing spondylitis. By embracing MRI, HLAB27 testing, and a broader set of clinical clues, they let us spot the disease earlier and treat it more effectively. Of course, every tool has limits costs, access, and the possibility of overdiagnosis remind us to stay balanced and patientcentered.
If youve found this guide helpful, why not print the quickcheck sheet, share your thoughts in the comments, or pass it on to someone who might need it? Were all in this together, learning, caring, and moving forward one step (or stretch) at a time.
FAQs
What are the main components of the eular criteria for ankylosing spondylitis?
The criteria require chronic low‑back pain ≥3 months starting before age 45, plus either MRI‑confirmed sacroiliitis or radiographic sacroiliitis together with a positive HLA‑B27 test. Supporting features such as elevated CRP, peripheral arthritis, uveitis, or a family history add diagnostic weight.
How does the 2022 update differ from the Modified New York criteria?
The 2022 ASAS‑EULAR update adds routine MRI use for early inflammation, lowers the CRP threshold, and incorporates peripheral manifestations. In contrast, the Modified New York criteria rely solely on plain‑film sacroiliitis and do not require HLA‑B27 or inflammatory markers.
Can a patient be diagnosed with ankylosing spondylitis without an MRI?
Yes. If clear radiographic sacroiliitis is present and the patient tests positive for HLA‑B27, the disease can be diagnosed using the older Modified New York criteria. However, MRI greatly improves sensitivity, especially in early or non‑radiographic cases.
What role does HLA‑B27 play in the eular criteria?
HLA‑B27 is a genetic marker that, when positive together with radiographic sacroiliitis, satisfies part of the classification. A positive test strengthens the likelihood of axial spondyloarthritis but is not mandatory if MRI shows definitive sacroiliac inflammation.
What are common pitfalls when applying the eular criteria?
Typical mistakes include relying only on X‑rays (missing early disease), misinterpreting MRI bone‑marrow edema that can appear in athletes or pregnancy, and overlooking peripheral signs such as enthesitis or uveitis that can tip the diagnosis in borderline cases.