If your joint suddenly aches, it could be the bodys reaction to an infection elsewhereor a direct infection inside the joint itself. Below we break down the key differences, symptoms, and treatment options so you can tell the two apart fast.
Quick Comparison Overview
| Feature | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Cause | Sterile inflammation triggered by an extraarticular infection (GI or GU) | Direct infection of the joint by bacteria, virus, or fungi |
| Onset | 14 weeks after primary infection | Hoursdays after bacteria enter the joint |
| Typical Joint(s) | Large lowerlimb joints (knee, ankle) | Any joint, often knee or hip |
| Systemic Signs | Mild fever, conjunctivitis, urethritis (the classic triad) | High fever, chills, marked leukocytosis |
| Synovial Fluid | Sterile, inflammatory | Purulent, positive culture |
| Prognosis | Usually selflimited (<6months) but can become chronic | Rapid joint destruction if untreated urgent care needed |
Seeing the contrast sidebyside helps you spot red flags faster. Remember, a quick decision can be the difference between a sore knee that heals and a joint that never fully recovers.
Pathophysiology Of Both
Reactive Arthritis Pathophysiology
Think of reactive arthritis as a misdirected army. An infection in your gut or urinary tract (commonly Chlamydia, Salmonella, Shigella) sends out bacterial fragments. Your immune system, especially if you carry the HLAB27 gene, mistakes those fragments for joint tissue and launches an attack.
Theres no actual germ in the joint the fluid stays sterile. The inflammation is driven by molecular mimicry, a fancy way of saying the enemy looks a lot like our own cells. For a deeper dive, see AS remission criteria.
Key Points to Remember
- Extraarticular infection precedes joint pain by 14 weeks.
- HLAB27 positivity increases risk and may predispose to chronicity.
- Synovial fluid is sterile culture will be negative.
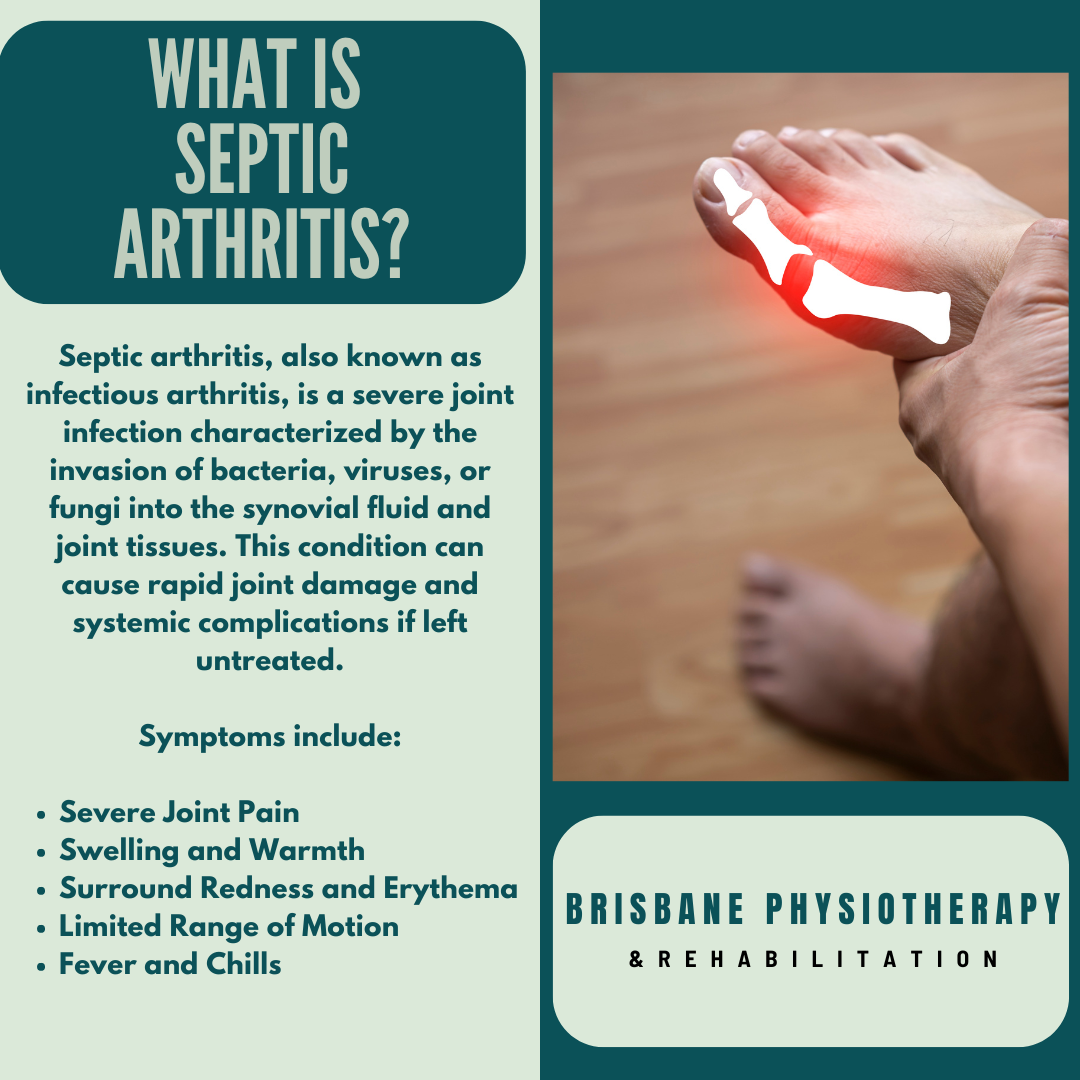
Septic Arthritis Pathophysiology
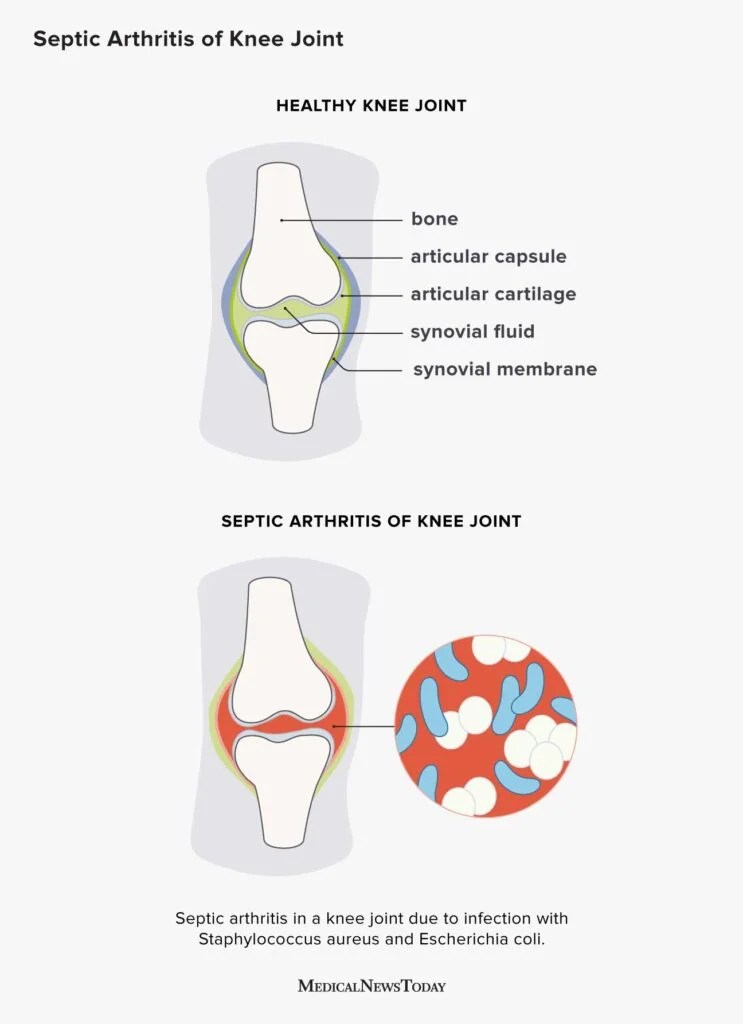
Septic arthritis is the opposite scenario: germs get a direct invitation into the joint space. The synovial membrane is highly vascular but lacks a robust barrier, allowing bacteria (most often Staphylococcus aureus) to multiply rapidly. The resulting pus swells the joint, destroys cartilage, and can spread to nearby bone thats where septic arthritis meets osteomyelitis.
Because the infection is intheroom, youll see a dramatic surge in white blood cells and a purulent fluid that lights up on Gram stain. Guidelines from stress immediate drainage to stop the damage.
Key Points to Remember
- Onset is abrupt pain, swelling, and fever can appear within hours.
- Common organisms: S. aureus, Streptococcus, N. gonorrhoeae.
- Joint aspiration yields pus; culture is usually positive.
Key Symptoms & Signs
What Youll Feel with Reactive Arthritis
Picture a modest, uneven ache that starts in one knee or ankle, hops over to the other side, and sometimes drifts up to the wrist. Add a touch of red eye (conjunctivitis) and a burning sensation when you pee thats the classic reactive arthritis triad.
Fever is usually lowgrade, and the joint swelling is more soft than explosive. The pain tends to linger for weeks, then slowly wanes.
What Youll Feel with Septic Arthritis
Now imagine a joint that feels like its been hit by a truck. The swelling is hard, the skin is hot, and the pain is so intense you cant bear weight. Fever spikes high, chills follow, and you might feel outright sick.
This isnt a slow burn its an emergency. If you suspect septic arthritis, call emergency services or head straight to the ER.
Diagnostic Workup Steps
Synovial Fluid Analysis
The gold standard for both conditions is joint aspiration. Heres what you typically see:
| Finding | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Cell Count (WBC/L) | 5,00020,000 (predominantly neutrophils) | >50,000 (predominantly neutrophils) |
| Gram Stain | Negative | Positive in 5070% of cases |
| Culture | Negative | Positive in 7090% of cases |
When the fluid looks cloudy and the count is high, youre leaning toward septic arthritis. If the test is sterile but the patient just recovered from a GI bug, think reactive.
Blood Tests & Imaging
Both conditions often raise ESR and CRP, but septic arthritis typically drives them higher. Blood cultures are essential if sepsis is suspected.
Plain Xrays might look normal early on; an ultrasound can catch effusion quickly, while MRI shines when you need to rule out osteomyelitis or assess cartilage loss.
Treatment Strategies Overview
Reactive Arthritis Treatment
First line? Good old NSAIDs ibuprofen or naproxen can tame the inflammation. If the pain sticks around, a short burst of corticosteroids (either oral or intraarticular) may be needed.
Most folks wonder, Do I need antibiotics? Only if the original infection persists (think chlamydia). Otherwise, antibiotics wont help the joint itself.
For chronic cases (about 10% of patients), rheumatologists may introduce DMARDs like sulfasalazine or a biologic, especially if HLAB27 is positive. The provide a clear algorithm.
SelfCare Tips
- Rest the affected joint but keep it moving gently (think light rangeofmotion exercises).
- Ice the swelling for 20 minutes, three times a day.
- Stay on top of the original infection finish any prescribed antibiotics.
Septic Arthritis Treatment
This is a race against time. The first step is urgent joint drainage either via needle aspiration, arthroscopy, or an open surgical washout. The goal is to remove pus and reduce pressure.
While youre waiting for cultures, start broadspectrum IV antibiotics (often vancomycin plus ceftriaxone) to cover MRSA, gramnegatives, and gonorrhea. Once you know the bug, narrow the regimen.
Dont forget about the bone. If the infection spreads, osteomyelitis can develop, especially in the hip or spine. In those cases, prolonged IV antibiotics (46 weeks) and possibly surgical debridement are required.
Safety Checklist
- Fever >38.5C, severe joint pain, or inability to bear weight go to the ER.
- Never delay aspiration; each hour of delay raises the risk of permanent damage.
- Follow up with orthopedics or rheumatology after discharge to ensure joint function returns.
Bottom Line Summary
Reactive arthritis is an immunemediated, usually selflimited joint inflammation that follows an infection elsewhere; septic arthritis is a true joint infection that demands immediate drainage and antibiotics. Knowing the hallmark signsthe triad of conjunctivitis, urethritis, and asymmetric arthritis for reactive, versus high fever, hot swollen joint, and purulent fluid for septichelps you act quickly.
Early recognition, proper joint aspiration, and targeted therapy can spare you from chronic pain or permanent joint damage. If you or someone you love experiences sudden joint pain with fever, urinary or eye symptoms, dont waittalk to a healthcare professional right away. Your joints will thank you.
FAQs
What are the main causes of reactive arthritis?
Reactive arthritis is triggered by an extra‑articular infection, most often gastrointestinal (e.g., Salmonella, Shigella) or genitourinary (e.g., Chlamydia) bacteria, and involves an immune reaction without bacteria in the joint.
How quickly does septic arthritis develop after infection?
Septic arthritis typically appears within hours to a few days after bacteria enter the joint space, causing rapid pain, swelling, and systemic signs like high fever.
Which joint fluid findings point to septic arthritis?
A synovial fluid WBC count > 50,000/µL, purulent appearance, positive Gram stain in 50‑70% of cases, and positive culture in 70‑90% are characteristic of septic arthritis.
When should antibiotics be used for reactive arthritis?
Antibiotics are only indicated if the preceding infection (e.g., chlamydia) is still active. They do not treat the joint inflammation itself.
What is the emergency treatment for septic arthritis?
Immediate joint drainage (needle aspiration, arthroscopy, or open washout) plus empiric intravenous antibiotics (e.g., vancomycin + ceftriaxone) until cultures identify the specific pathogen.