Why Radiology Matters
What does radiology reveal that surgery cant?
During an operation the surgeon can see the ovary and any obvious spread, but they cant look deep into the abdomen without opening it up. RadiologyCT, MRI, PETCTgives a birdseye view of the whole pelvis and abdomen, showing hidden nodules, fluid collections, and lymphnode involvement. This noninvasive snapshot helps determine if a tumor is resectable, if additional therapy is needed before surgery, or if a different surgical approach is warranted.
How does imaging shape your treatment plan?
When the radiology report aligns with the FIGO (International Federation of Gynecology and Obstetrics) staging criteria, oncologists can choose the right blend of surgery, chemotherapy, and, when appropriate, targeted therapy. For instance, a stageIIIC findinglarge peritoneal implants or bulky nodesusually means neoadjuvant chemotherapy first, followed by interval debulking surgery. Without precise imaging, you could end up with an unnecessary extensive operation or delayed systemic treatment.
Key metrics radiologists look for
- Size of the primary ovarian mass
- Capsular rupture or tumor spill
- Presence of peritoneal implants
- Lymphnode enlargement (pelvic, paraaortic)
- Ascites volume and distribution
FIGO Staging Basics
What are the current FIGO stages and their radiologic criteria?
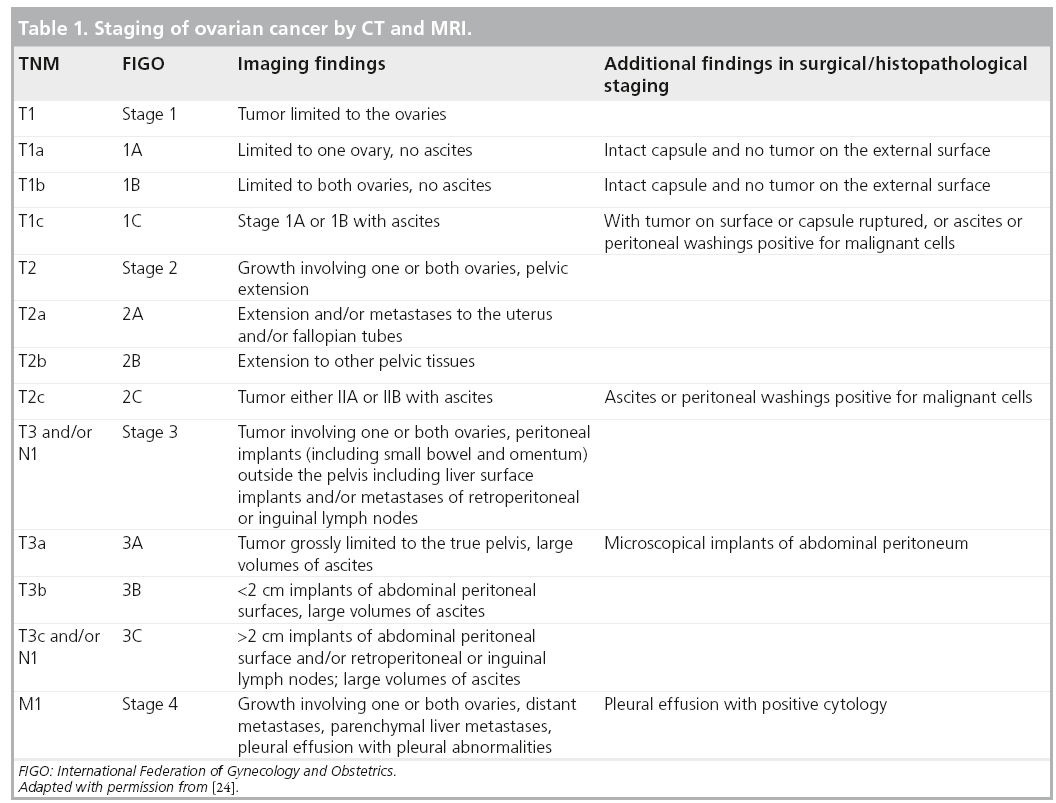
The FIGO staging system (latest revision 2014, still current in 2024) categorizes ovarian cancer from stageI (confined to ovaries) through stageIV (distant metastasis). Radiologic criteria for each stage are:
- StageI: Tumor limited to one or both ovaries, no extraovarian disease on CT or MRI.
- StageII: Involvement of the pelvis (uterus, fallopian tubes) or the peritoneum outside the pelvis, identifiable as softtissue implants on imaging.
- StageIII: Peritoneal implants outside the pelvis and/or regional lymphnode metastasis; bulky disease often seen as masses >2cm.
- StageIV: Distant metastasis to liver parenchyma, lungs, or other organsusually picked up on PETCT or contrastenhanced CT.
What changed in the 2014 revision and are there 2024 updates?
The 2014 update clarified the distinction between microscopic and macroscopic spread and added the importance of nodal involvement. While a formal 2024 revision hasnt been published yet, several societies (e.g., ESUR) have issued clinical practice updates that emphasize using diffusionweighted MRI for better detection of peritoneal implants. You can download the official FIGO PDF for the exact wording.
FIGO Stage vs. Typical Imaging Findings
| FIGO Stage | Typical CT/MRI Findings |
|---|---|
| I | Unilateral or bilateral ovarian mass, smooth capsule, no extraovarian lesions |
| II | Mass extending to uterus or pelvic peritoneum; small peritoneal nodules |
| III | Peritoneal implants >2cm, retroperitoneal lymphnode enlargement, ascites |
| IV | Liver parenchymal mets, pleural effusion, lung nodules on PETCT |
Imaging Options Explained
Which modality is firstline for staging?
For most patients, a contrastenhanced multidetector CT (MDCT) is the workhorse. Its fast, widely available, and excellent at showing lymphnode size, ascites, and organ involvement. MRI, especially with diffusion weighting, steps in when CT is equivocal or when radiation exposure is a concernthink younger patients or those needing fertilitysparing surgery. PETCT is reserved for suspected distant disease or for monitoring treatment response.
Can a radiology assistant (AI or technologist) improve accuracy?
Emerging AI tools can automatically highlight suspicious lesions, calculate tumor volume, and even suggest a FIGO stage. Early studies show a 1015% boost in detection of small peritoneal implants when AI assistance is used. While not a replacement for a skilled radiologist, these assistants act like a second pair of eyeshelpful, especially in busy centers.
Imaging Modality Comparison
| Modality | Preferred When | Strengths | Limitations / Risks |
|---|---|---|---|
| CT (MDCT) | Initial surgical planning | Rapid, excellent nodal & ascites assessment | Radiation dose |
| MRI (incl. DWI) | Equivocal CT or fertilitysparing cases | Superior softtissue contrast, no radiation | Longer exam, higher cost |
| PETCT | Assessing distant mets or recurrence | Functional metabolic info | Limited for tiny peritoneal implants, radiation |
| Transvaginal Ultrasound | Initial detection & biopsy guidance | Realtime, no radiation | Operatordependent, limited staging scope |
Reading Scan Reports
How to interpret a CT report for ovariancancer staging?
Most radiology reports follow a structured format:
- Technique: Type of scan, contrast used.
- Findings: Description of the ovarian mass, size, capsule integrity, and any extraovarian disease.
- Impression: The radiologists summary, often stating a suggested FIGO stage.
Look for key phrases like no evidence of distant metastasis, bulky retroperitoneal nodes, or ascites moderate. If anything feels unclear, dont hesitate to ask your oncologist for clarificationWhat does 'bulky' mean for my case?
What does nonresectable disease look like on imaging?
Typical signs include:
- Encasement of major vessels (aorta, vena cava) by tumor
- Masses >10cm that infiltrate multiple organ surfaces
- Extensive diaphragmatic or hepatic peritoneal implants
These findings usually shift the plan toward neoadjuvant chemotherapy first.
Case Vignette
Sarah, 58, presented with bloating and was found to have a 9cm left ovarian mass. CT showed thickened omentum, bilateral pelvic nodes measuring 2.5cm, and moderate ascites. The radiologists impression: StageIIIC disease, likely nonresectable at this time. After three cycles of carboplatinpaclitaxel, repeat imaging showed shrinkage of nodes and the tumor became operable, allowing a successful interval debulking.
Benefits and Risks
What are the benefits of accurate radiologic staging?
Precise staging guides the right treatment intensity, sparing you from overly aggressive surgery if it wont help, while ensuring you get enough chemotherapy when needed. It also gives a realistic prognosis, helping you plan ahead with your family and care team.
What risks should I be aware of?
Every imaging test carries some tradeoff:
- CT: Radiation exposurethough modern lowdose protocols keep it well below harmful levels ().
- MRI: May be uncomfortable for claustrophobic patients; gadolinium contrast can rarely affect kidney function.
- PETCT: Additional radiation from the radiotracer, and falsepositive uptake in inflammatory tissue.
Discuss any concerns with your radiology team; they can tailor protocols to minimize risk.
RiskMitigation Strategies
- Choose MRI for younger patients when feasible.
- Ask for lowdose CT protocols if multiple scans are planned.
- Ensure proper hydration before and after contrast administration.
Radiology Assistant Role
Who is the radiology assistant?
In a modern imaging department, the assistant can be a highly trained technologist who prepares the patient, optimizes scan parameters, and ensures highquality images. More recently, software platforms act as assistants, automatically segmenting masses and measuring volumes.
How does the assistant fit into the multidisciplinary team?
After the scan, the radiologist presents the findings at a tumor board alongside surgeons, medical oncologists, and pathologists. The assistant may provide additional technical detailslike contrast timingor share AIgenerated measurements that help the team reach a consensus faster.
Typical Workflow
- Patient checkin fasting & consent.
- Technologist (assistant) sets up protocol.
- Scan performed images sent to PACS.
- Radiologist reviews, optionally using AI assistance.
- Report entered & discussed at tumor board.
- Treatment plan finalized.
Practical Patient Tips
How should I prepare for my staging scan?
Good preparation makes the images clearer and the experience smoother:
- Fast for at least 46hours if contrast is used.
- Bring a list of medications and any allergy history (especially to iodine or gadolinium).
- Wear comfortable, metalfree clothing.
- Stay hydrateddrink water before and after the exam.
Questions to ask your radiologist
Dont be shyhere are some plainspoken questions you can ask:
- What FIGO stage does the imaging suggest?
- Are there any findings that could change my surgical plan?
- Is there a need for additional imaging, like MRI, to confirm any ambiguous spots?
- What are the radiation doses, and can they be reduced?
Downloadable Staging Checklist
For easy reference, you can print a (PDF) to bring to your appointment. It includes space to note the imaging modality, key findings, and any questions you have.
Future Advances
How is AI reshaping ovariancancer staging?
Early pilot studies demonstrate AI algorithms that can automatically calculate tumor volume, detect subcentimeter peritoneal nodules, and suggest a FIGO stage with 8590% accuracy. While still under validation, these tools promise to reduce interobserver variability and speed up reporting.
What about radiomics and molecular imaging?
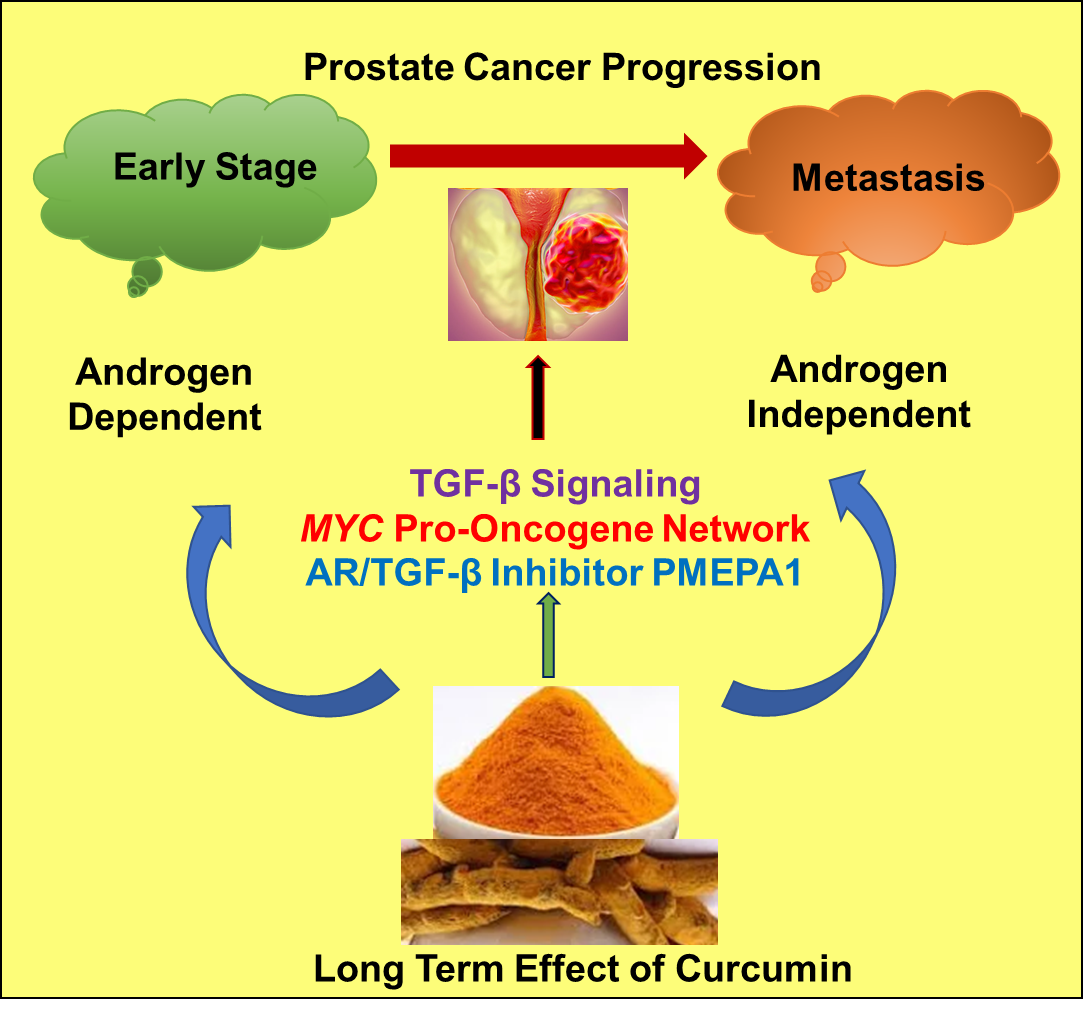
Radiomics extracts hundreds of quantitative features from images (texture, shape, intensity) that can predict tumor biology and chemotherapy response. Combined with PET tracers targeting specific molecular pathways, doctors may soon personalize therapy based not just on stage, but on the tumors unique fingerprint. For patients also navigating cancer beyond gynecologic cancers, resources about broader topics like prostate cancer outlook can help compare how imaging and prognosis differ by cancer type.
Potential impact on FIGO revisions
Experts anticipate that the next FIGO update could incorporate quantitative imaging biomarkerslike apparent diffusion coefficient (ADC) values from MRIto refine stageII versus stageIII distinctions. Staying informed about these trends can empower you to ask your care team about emerging options.
Conclusion
Radiology is the compass that guides every step of ovariancancer treatmentfrom pinpointing the exact FIGO stage to deciding whether you go straight to surgery or start with chemotherapy. Understanding the strengths and limits of each imaging modality, asking the right questions, and collaborating with a multidisciplinary team puts you in the drivers seat of your care. Keep this guide handy, talk openly with your doctors, and remember that the right images today can chart a clearer, healthier tomorrow.
FAQs
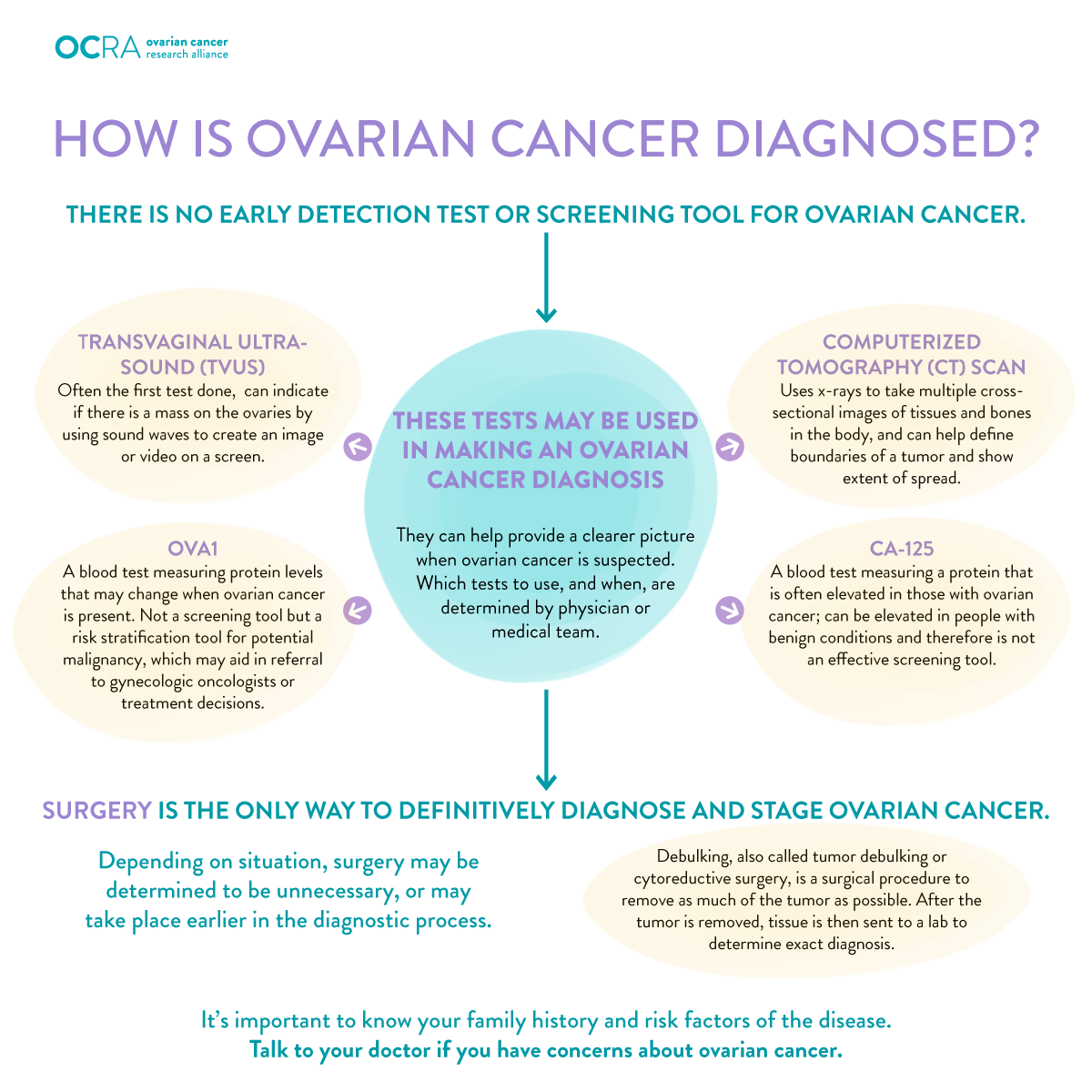
What is the role of radiology in ovarian cancer staging?
Radiology provides detailed images through CT, MRI, and PET-CT scans that reveal tumor size, spread to lymph nodes, peritoneal implants, and distant metastasis, enabling accurate staging beyond what surgery alone can determine.
Which imaging modality is preferred first for staging ovarian cancer?
Contrast-enhanced multidetector CT (MDCT) is typically the first-line imaging choice due to its speed, availability, and ability to detect lymph node involvement, ascites, and organ metastases.
How does radiology impact treatment planning for ovarian cancer?
Imaging findings aligned with FIGO staging help oncologists tailor treatment, deciding between surgery first or neoadjuvant chemotherapy followed by interval debulking, optimizing patient outcomes.
Can AI improve the accuracy of ovarian cancer staging in radiology?
Yes, emerging AI tools assist radiologists by automatically detecting small tumor implants, calculating tumor volumes, and suggesting stages, improving detection rates and reporting efficiency.
What are the risks associated with ovarian cancer staging imaging?
Potential risks include radiation exposure from CT and PET-CT scans and rare side effects from contrast agents used in MRI; protocols are tailored to minimize these risks, especially in younger patients.