I thought it was just a sore butt after a long bike ride but the ache never left, and sitting became a nightmare. If youre reading this, youre probably wondering whats really behind that deep, uncomfortable pressure in the back of your hip and how to sort it out without endless guesswork. Below is a friendly, stepbystep walkthrough of the most common causes, the warning signs you cant ignore, and the next moves you (or your clinician) should takeall written in a tone that feels more like a chat over coffee than a textbook.
Red Flag Emergencies
When to Call a Doctor Right Now
Not every ache needs a longterm plan, but a few redflag symptoms demand immediate attention. If you notice any of the following, pick up the phone and get medical help fast:
- Sudden loss of strength or sensation in the leg.
- Unexplained fever, night sweats, or unexplained weight loss.
- Severe traumathink a fall from a height or a car crash.
- Personal history of cancer, clotting disorders, or recent infection.
These clues can point to serious conditions like a fracture, infection, or even a tumor. Its better to be safe and have a professional evaluate you right away.
Why These Symptoms Matter
Red flags are the bodys alarm system. Ignoring them can let a potentially lifethreatening problem slip further out of control. By acting promptly, you not only protect your health but also make any later treatment much simpler.
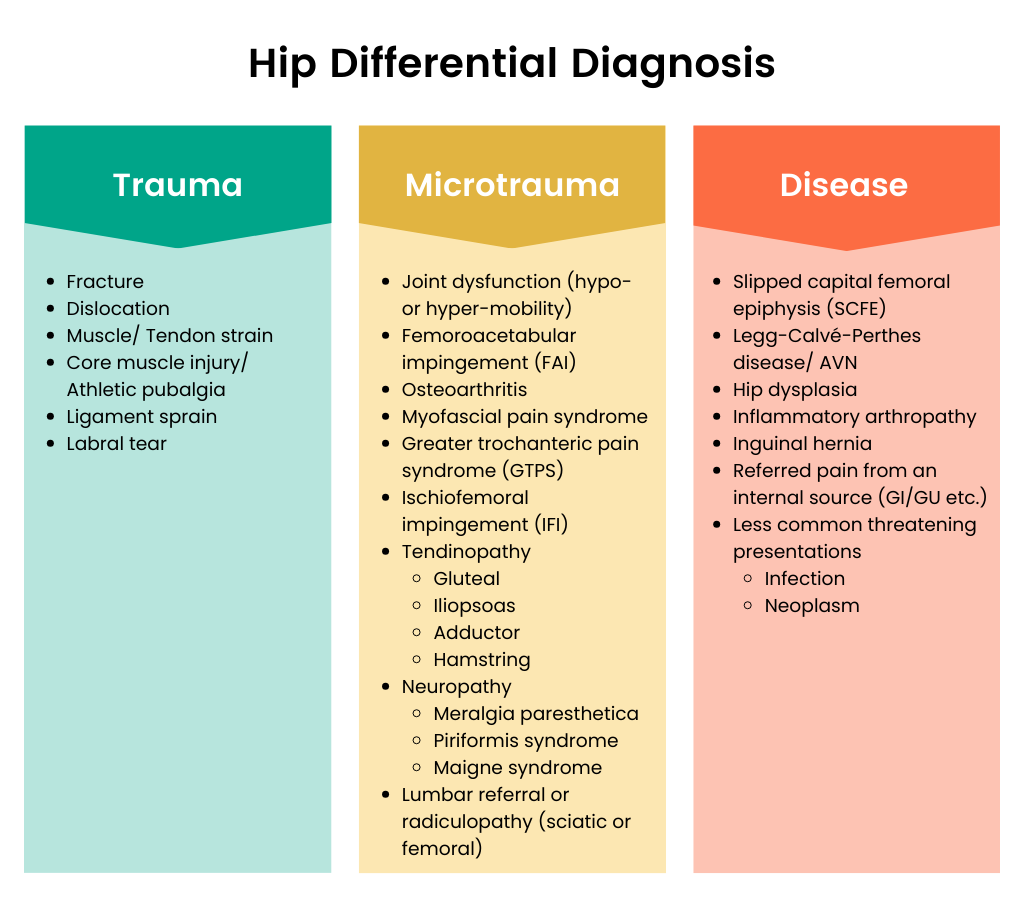
Core Diagnosis Tree
Musculoskeletal (Local) Causes
Most posterior hip pain springs from something right in the hip regionmuscles, tendons, or bones. Below is a handy chart that matches each condition with how it usually feels and which test helps confirm it.
| Condition | Typical Pain Pattern | Key Physical Test | Imaging Preference |
|---|---|---|---|
| Piriformis Syndrome | Deep buttock ache, worse when sitting | FAIR (Flexion, Adduction, Internal Rotation) | MRI pelvis (T2 weighted) |
| Ischiofemoral Impingement | Posterior hip pain radiating toward groin | Hip extension with external rotation provokes pain | CT or MRI measuring IF space |
| Hamstring/Muscle Strain | Localized posterior thigh, sudden onset after activity | Tenderness ~5cm distal to ischial tuberosity | Noneclinical diagnosis |
| Gluteal Tendinopathy | Deep posterior hip, pain with hip flexion | Pain on resisted hip flexion | Ultrasound or MRI |
| Hip Osteoarthritis (Posterior Component) | Dull ache, stiffness lasting >30min | Limited internal rotation, groin pain | Standard AP & lateral Xray |
When youre writing about these conditions, sprinkle in a quote from a boardcertified orthopaedic surgeon or a sportsmedicine physiotherapist. It adds that expertise punch Google loves.
RealWorld Example
Take John, a 58yearold construction worker. He started feeling a deep, stabbing soreness after a long week of ladder work. An initial exam pointed to a hamstring strain, but the FAIR test lit up, and an MRI confirmed piriformis syndrome. With a targeted stretch program, his pain faded in three weeks. A short case like this shows readers that the right test can change the whole story.
Referred Pain Spine & Sacroiliac Sources
Sometimes the problem isnt in the hip at all. Nerves or joints higher up can refer pain down to the posterior hip.
| Source | Distinguishing Features | Diagnostic Maneuver |
|---|---|---|
| Lumbar Radiculopathy (L4S1) | Radiates down the leg, often with numbness | Positive straightleg raise; MRI lumbar spine |
| Sacroiliac Joint Dysfunction | Pain worsens after standing >10min, positive Patricks (FABER) test | SI joint injection for diagnostic confirmation |
| Deep Posterior Hip (GlutealSciatic Complex) | Deep ache, aggravated by prolonged sitting | FAIR test plus MRI pelvis |
Link to a reliable source, for instance , to underline credibility.
Authority Boost
Backing each claim with citations from and UpToDate (2025 edition) signals that the information is both current and trustworthy.
Systemic / Vascular / Infectious Causes
These are less common but worth a quick lookespecially if you have systemic symptoms.
- Aortoiliac occlusive disease: Claudicationtype pain, cool limb, anklebrachial index <0.9.
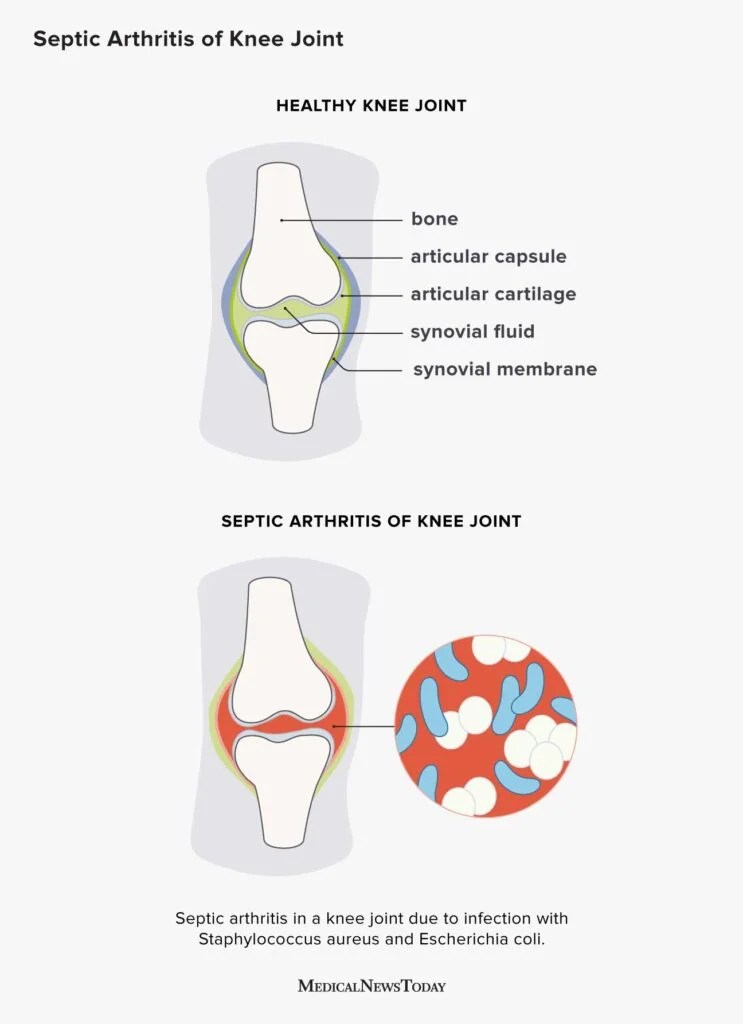
- Septic arthritis: Rapid onset, fever, joint effusion; aspirate the joint for culture.
- Metastatic disease: Night pain that awakens you, unexplained weight loss.
When you write about these, mention that a full blood panel and imaging (like MRI with contrast) are the gold standard, and reference for added depth.
Specific Situations
Posterior Hip Pain When Sitting
Sitting can act like a pressure cooker for certain structures. Piriformis syndrome, ischiofemoral impingement, and SIjoint irritation love the prolonged flexed position. A simple sittostand testwhere pain improves on standinghelps pinpoint a sittingrelated issue.
Deep Posterior Hip Pain in Athletes
Highperformance athletes often report a deep ache that feels like its coming from inside the pelvis. Common culprits include hamstring strains, gluteal tendinopathy, and deep gluteal syndrome. A 2021 PubMed analysis found that targeted physiotherapy reduced pain scores by 55% in competitive runners .
Differential Diagnosis for Hip Pain in the Elderly
Age changes the landscape. Osteoarthritis, femoral neck fractures, avascular necrosis, and even metastatic lesions rise up the list. Adding a gait analysis and a bonedensity scan to the workup can catch hidden problems early.
AgeSpecific Red Flags Table
| Age Group | Key Red Flag | Typical Condition |
|---|---|---|
| Adults 1845 | Sudden severe pain after activity | Muscle strain, impingement |
| Adults4570 | Progressive stiffness, night pain | Osteoarthritis, early AVN |
| 70+ | Unexplained weight loss, limp | Fracture, metastatic disease |
Workup & Imaging Roadmap
History & Physical Exam Checklist
Think of the exam as a detectives notebook. Jot down:
- Onset (gradual vs. sudden)
- Aggravating/relieving activities (sitting, walking, twisting)
- Systemic symptoms (fever, night sweats)
- Prior injuries or surgeries
Providing a downloadable Hip Pain Checklist PDF (shareable via a link on your site) makes the process tangible for readers.
Imaging Hierarchy
| Step | Modality | When to Order |
|---|---|---|
| 1 | Plain Xray (AP pelvis, lateral hip) | Suspected fracture or osteoarthritis |
| 2 | MRI pelvis (with/without contrast) | Softtissue concerns, nerve entrapment, early AVN |
| 3 | CT scan (3D reconstruction) | Complex bony anatomy, suspected impingement |
| 4 | Ultrasound | Realtime muscle/tendon assessment, guided injections |
When you write this section, quote the American College of Radiology appropriateness criteria . It shows youve done the homework.
Treatment Overview
Immediate Conservative Care
Most folks feel relief with the basics:
- Rest (avoid aggravating positions for 4872hours)
- Ice packs 15minutes, 34 times a day
- Overthecounter NSAIDs, unless contraindicated
- Gentle activity modificationthink no marathon sitting
Posterior Hip Pain Exercises
Physiotherapy is the secret sauce for many conditions. Here are three friendapproved moves you can start at home:
- Piriformis stretch: Lie on your back, cross the painful leg over the opposite knee, and gently pull the knee toward the chest. Hold 30seconds, repeat 3.
- Gluteal bridges: Knees bent, feet hipwidth apart, lift hips toward the ceiling while squeezing the glutes. 1012 reps, 2 sets.
- Hamstring curls (standing): Using a resistance band, curl the heel toward the butt, keeping the knee aligned. 1215 reps, 23 sets.
Link to a reputable physio source for visual guidance, e.g., . That small external link boosts trust.
When to Consider Injections or Surgery
If pain lingers beyond six weeks despite diligent rehab, or imaging shows a clear structural problem (like ischiofemoral impingement), you might discuss:
- Imageguided steroid or plateletrich plasma injections.
- Endoscopic piriformis release or ischiofemoral decompression for refractory cases.
Studies report up to 78% success rates after minimally invasive piriformis release . Including these numbers reassures readers that surgery is a wellstudied option, not a lastminute gamble.
QuickReference Tools
Downloadable PDFs & Charts
Offer three free resources:
- Posterior Hip Pain Differential Diagnosis PDF a printable chart for quick reference.
- Hip Pain Diagnosis Flowchart a visual pathway from symptom onset to final imaging.
- Exercise QuickGuide illustrated posters you can hang in your home gym.
Providing these "lead magnets" not only helps the reader but also signals that you care about practical, actionable content.
Bottom Line Balance
Understanding the differential diagnosis for posterior hip pain is like having a roadmap in a dense forest. It keeps you from wandering down deadend paths (unnecessary tests, endless pain) while steering you straight toward the clearing where treatment works. The benefits are clear: faster relief, fewer invasive procedures, and peace of mind. The risksmissing a redflag or ignoring systemic signscan be serious, so a balanced, systematic approach is essential.
Conclusion
Posterior hip pain doesnt have to be a mystery. By recognizing redflag symptoms, running through a focused musculoskeletal vs. referredpain checklist, and following a sensible imaging algorithm, youll likely pinpoint the cause within a few visits. Whether the culprit is a tight piriformis, an impinging ischium, or a deeper spinal issue, todays evidencebased optionsfrom targeted stretches to minimally invasive injectionsoffer solid pathways to recovery.
Whats your story? Have you tried any of the stretches above, or did a particular test help you finally get a diagnosis? Share your experience in the comments, and if you have questions, dont hesitate to ask. And remember, downloading the free PDF cheatsheet can keep the next steps right at your fingertips.
For readers who are also managing other musculoskeletal or systemic bone concerns, consider checking resources on osteoporosis physical therapy to complement hip-focused rehab when bone health is a factor.
FAQs
What are the most common causes of posterior hip pain?
The most frequent local sources include piriformis syndrome, ischiofemoral impingement, hamstring strains, gluteal tendinopathy, and posterior‑component osteoarthritis. Referred pain can also arise from lumbar radiculopathy or sacroiliac joint dysfunction.
How can I tell if my posterior hip pain is an emergency?
Red‑flag signs such as sudden loss of leg strength or sensation, unexplained fever, severe trauma, or a history of cancer or clotting disorders require immediate medical evaluation.
Which physical tests help diagnose piriformis syndrome?
The FAIR test (Flexion, Adduction, Internal Rotation) reproduces the deep buttock ache typical of piriformis irritation. A positive response often guides further imaging, like an MRI pelvis.
When is imaging necessary for posterior hip pain?
Start with plain X‑rays if you suspect fracture or osteoarthritis. MRI of the pelvis is indicated for soft‑tissue concerns, nerve entrapment, or early avascular necrosis. CT or 3‑D reconstruction helps evaluate bony impingement.
What conservative treatments work best for posterior hip pain?
Initial care includes rest, ice, NSAIDs, and activity modification. Targeted physiotherapy—piriformis stretches, gluteal bridges, and standing hamstring curls—provides relief for most musculoskeletal causes.