Got your thyroid removed and now wondering what comes next? In a nutshell, the journey after a papillary thyroidectomy usually means three things: lifelong hormone replacement, a decision about radioactive iodine (RAI) and a plan for steady monitoring. Knowing why each step matters, what the possible sideeffects are, and how you can stay on top of things will help you feel in control rather than stuck in whatnow limbo.
Immediate PostOp Steps
How hormone replacement begins
Right after the surgeon closes the incision, youll start taking levothyroxinea synthetic version of the thyroid hormone you just lost. Most endocrinologists kick off with a dose of about 1.6g per kilogram of body weight, split into a single morning tablet. The idea is to mimic the hormone levels your thyroid used to produce, keeping your metabolism humming along.
Dont be surprised if your doctor asks you to come back in 46weeks for a TSH (thyroidstimulating hormone) check. Thats the goldstandard test that tells you whether the dose is spoton, too low (leading to fatigue, weight gain) or too high (causing jittery nerves, heart palpitations). Adjustments are normal; think of it as finetuning a radio until you get the clearest signal.
When is radioactive iodine (RAI) recommended?
RAI isnt a blanket requirement for everyone. The American Thyroid Association () suggest it for patients with intermediate or highrisk diseasebasically when the tumor was larger than 4cm, there was spread to lymph nodes, or the pathology shows aggressive features.
If you fall into that group, youll likely receive a single dose of 30150mCi of I131 about 46weeks after surgery, once your TSH is enough to pull the iodine into any leftover thyroid cells. Most people tolerate it well, though you may notice a dry mouth or taste changes for a few weeks. The upside? It can wipe out microscopic disease that you cant see on imaging.
What are the immediate postop sideeffects?
Even with a smooth operation, there are a few hiccups you might run into:
- Voice changes: A sore throat or hoarseness can happen if the recurrent laryngeal nerve was brushed. Its usually temporary, but if it lingers, a speech therapist can help.
- Calcium drops: The parathyroid glands sit right next to the thyroid and can be bumped during surgery, leading to low calcium. Your surgeon will often give calcium supplements for a short period.
- Neck discomfort: Swelling and stiffness are common for the first couple of weeks. Gentle neck stretches (as your doctor advises) can speed up recovery.
How long will I need thyroid hormone pills?
Because the thyroid is gone for good, levothyroxine is a lifelong companion. That sounds daunting, but once you find the right dose, it becomes as routine as a morning coffee. During pregnancy, older age, or if you start a new medication that interferes with absorption, your dose might need tweaksso keep an open line with your endocrinologist.
LongTerm Management
What labs and imaging are required for followup?
Surveillance is the secret sauce that lets you and your doctor catch any recurrence early. Heres a typical schedule:
| Time after surgery | Test/Imaging | Purpose |
|---|---|---|
| 6weeks | TSH, free T4 | Confirm hormone dosing |
| 36months | Thyroglobulin (Tg) & antiTg antibodies | Baseline tumor marker |
| 6months | Neck ultrasound | Look for residual tissue or lymph node involvement |
| 12months onward (annually) | Tg + ultrasound | Ongoing monitoring |
Thyroglobulin is a protein that thyroid cells make; after a total thyroidectomy, a detectable Tg can signal leftover or recurring disease. Pair it with a neck ultrasound, and you have a powerful, noninvasive combo.
How is remission defined?
In the thyroid world, remission usually means an undetectable Tg level (or <0.2ng/mL with a sensitive assay) and a clean ultrasound for at least 12months. If you hit that milestone, the odds of the cancer coming back drop dramaticallythink below 5% for lowrisk patients.
When is additional RAI needed?
If your Tg starts creeping up or a new spot shows up on ultrasound, your doctor may recommend a second RAI dose. The decision hinges on the size of the residual tissue, the aggressiveness of the original tumor, and your overall health. Its never a onesizefitsall callyour care team will weigh the benefits against the modest risk of secondary malignancies from extra radiation.
What are the signs of recurrence?
Stay alert for any of these red flags:
- New lump or swelling in the neck
- Persistent hoarseness or difficulty swallowing
- Unexplained weight loss or night sweats
- Sudden change in energy levels, even if your hormone levels look normal
If anything feels off, reach out to your endocrinologist promptly. Early detection makes treatment far easier.
How does staging affect followup?
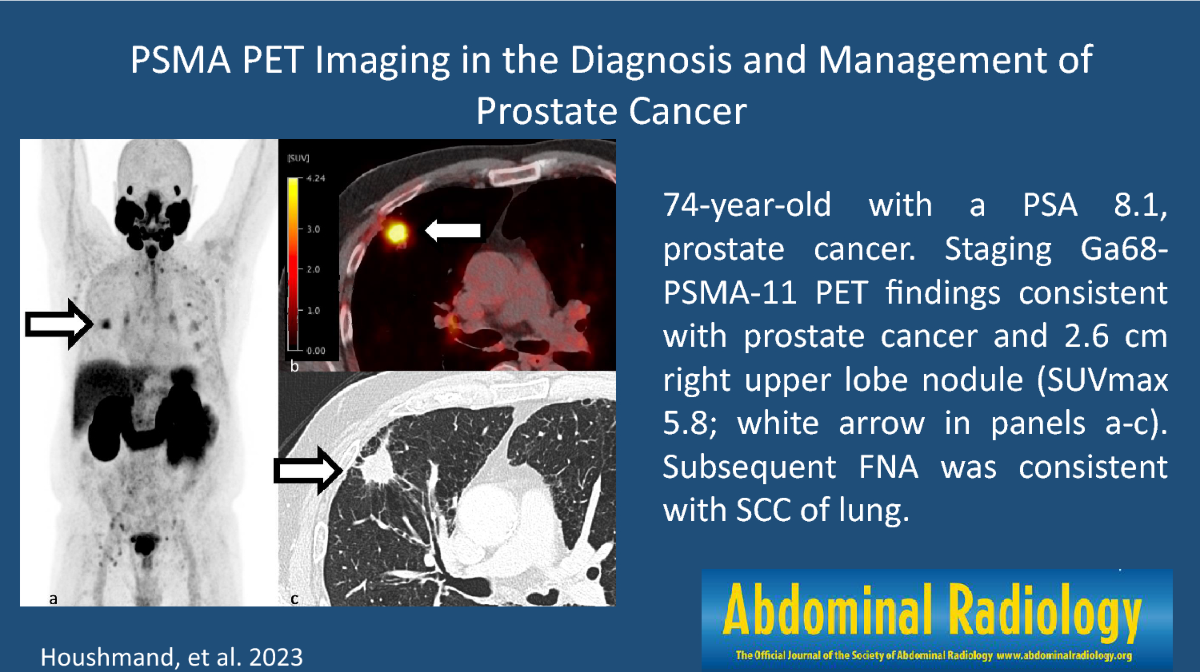
Staging, as laid out in the papillary thyroid carcinoma staging system, groups patients from StageI (small, confined tumors) to StageIV (distant metastasis). For StageI disease, the followup schedule can be more relaxedannual labs and ultrasound may suffice. For higher stages, especially metastatic papillary thyroid carcinoma, imaging may include a wholebody scan, CT, or PET, and the interval between visits shortens to every 36months.
Alternatives & Adjuncts
Can papillary thyroid cancer be treated without surgery?
Yes, but only for a very select group. When a papillary microcarcinoma (1cm) is discovered incidentally and shows no aggressive features, active surveillance becomes an option. Studies from Japan have shown that only about 5% of these small lesions grow significantly over 10years, and most patients avoid surgery altogether.
What about nonsurgical therapies?
When surgery isnt feasibleperhaps because the tumor has invaded vital structuresor when disease recurs despite prior surgery, other tools step in:
- External beam radiation: Rarely used, reserved for unresectable, locally advanced tumors.
- Targeted kinase inhibitors: Drugs like lenvatinib and sorafenib have become the goto for metastatic papillary thyroid carcinoma that no longer responds to RAI. They work by blocking the pathways that fuel tumor growth.
- Radiofrequency ablation or ethanol injection: Minimally invasive techniques for isolated nodules that cant be removed surgically.
How do guidelines address thyroid cancer treatment without surgery?
The NCCN and ATA both note that, while surgery remains the cornerstone, nonsurgical management may be considered in highly selected casesespecially for patients with contraindications to anesthesia or for very lowrisk microcarcinomas. The key is shared decisionmaking, where your values, lifestyle, and risk tolerance shape the plan.
Balancing Benefits & Risks
What are the main benefits of postsurgical treatment?
When everything alignsappropriate hormone dosing, selective RAI, diligent monitoringyoure looking at a nearcure scenario. The 20year survival rate for stageI papillary thyroid cancer is over 95% (), meaning most patients live long, healthy lives after treatment.
What risks should patients weigh?
Every benefit comes with a flip side:
- RAI sideeffects: Dry mouth, altered taste, and in rare cases, a slight increase in second primary cancers.
- Levothyroxine overreplacement: Too much hormone can cause palpitations, anxiety, and bone loss over time.
- Underreplacement: Fatigue, weight gain, depressionnothing you want.
Thats why regular labs and open conversations with your doctor are nonnegotiable.
How to discuss options with your endocrinologist?
Walk into the appointment armed with a checklist:
- Current dose of levothyroxine and recent TSH result.
- Any symptomsnew hoarseness, calcium tingling, weight changes.
- Questions about RAI: Do I need another dose? What will the sideeffects be?
- Future plans: pregnancy, travel, new medications.
- Longterm monitoring: How often should I get ultrasounds and Tg tests?
Having these points written down helps the conversation stay on track and shows youre an active partner in your care.
Realworld case study: A new moms Dilemma
Sarah, a 32yearold mother of a newborn, faced a tough decision after her thyroidectomy. Her doctor recommended RAI, but she was worried about lactation. Together they chose to postpone RAI until after breastfeeding, while keeping hormone levels tight and doing close Tg checks. Six months later, after weaning, Sarah completed a lowdose RAI and is now thrivingher child is healthy, and her cancer markers stay negative. Stories like Sarahs highlight that treatment plans can be flexible when youre honest about life circumstances.
Resources & Tools for Patients
Feeling a bit overwhelmed? Here are some freebies you can grab right now:
- PostSurgery Care Checklist: A printable list of labs, medication doses, appointment reminders, and symptom trackers.
- Trusted Websites: American Cancer Society, American Thyroid Association, and Mayo Clinic all have uptodate, evidencebased info.
- Support Communities: Online forums like the Thyroid Cancer Survivors Network or local hospital support groups can connect you with folks walking the same path.
Remember, this guide is educationalnot a substitute for personalized medical advice. Always run any decision past your healthcare team.
Conclusion
After a thyroidectomy, the road ahead is all about balance: a steady dose of hormone replacement, the right use of radioactive iodine when needed, and vigilant monitoring to catch any whispers of recurrence. Understanding the why behind each step turns anxiety into empowerment, and the excellent 20year survival rates for papillary thyroid cancer show that most people go on to live full, vibrant lives. Grab the free postoperative checklist, join a community of survivors, and keep the conversation open with your doctoryouve got a solid plan, and youre not alone on this journey.
For patients also navigating cancer risks in other organs, it can help to review related followup and lifestyle guidance for example, guidance on colon cancer genetic testing can inform family screening conversations that sometimes overlap with thyroid cancer care.
FAQs
What is the role of hormone replacement after papillary thyroid cancer surgery?
After thyroid removal, patients start lifelong levothyroxine therapy to replace thyroid hormone and maintain metabolic balance. The dose is regularly adjusted based on TSH levels for optimal effect.
When is radioactive iodine (RAI) treatment recommended after surgery?
RAI is advised mainly for patients with intermediate to high risk features such as tumors over 4 cm, lymph node involvement, or aggressive cancer types, usually given 4-6 weeks post-surgery to ablate residual cells.
How is remission defined following papillary thyroid cancer treatment?
Remission is typically defined as an undetectable thyroglobulin (Tg) level combined with a clear neck ultrasound for at least 12 months, indicating a very low risk of cancer recurrence.
What are common side effects immediately after papillary thyroid cancer surgery?
Patients may experience temporary voice changes, low calcium levels due to parathyroid impact, and neck discomfort or swelling, all usually manageable and transient.
How frequently should monitoring tests occur after surgery?
Typical follow-up includes TSH and free T4 testing about 6 weeks post-op, Tg and anti-Tg antibodies every 3-6 months initially, neck ultrasounds annually, and more frequent imaging for higher-stage disease.