Quick answer: Migratory arthritis can usually be calmed with a blend of NSAIDs, shortterm steroids, gentle physical therapy, and an antiinflammatory diet. Most folks feel better within a few weeks, but the exact timeline hinges on whats causing the joint hopping.
What youll get: A friendly walkthrough of why the pain jumps around, how doctors pin down the cause, which treatments work best, what to eat, and the moments you should call a rheumatologist. Lets dive in, shall we?
What Is Migratory Arthritis?
How is it defined?
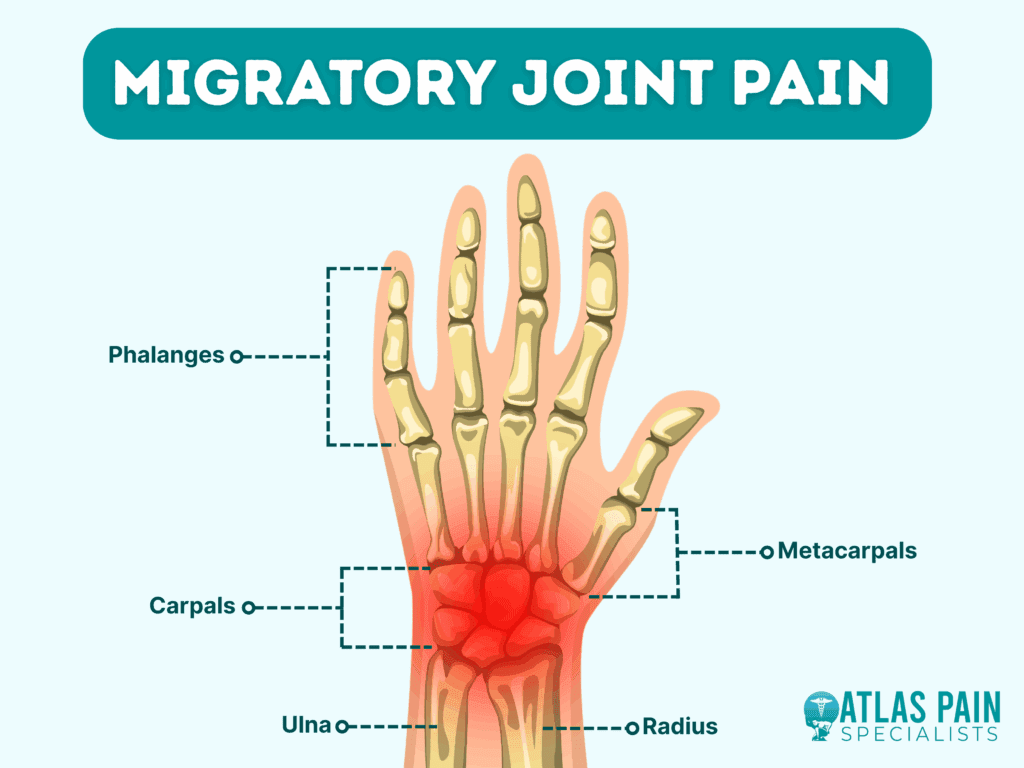
In plain terms, migratory arthritis is when swelling and pain hop from one joint to anotheroften within 2448hoursrather than staying put. Think of it like a traveler that never stays in one city for long.
How does it differ from other arthritis?
Unlike rheumatoid arthritis, which tends to affect the same joints symmetrically for months, migratory arthritis is fleeting. Palindromic rheumatism also moves around, but its episodes are usually shorter (minutes to hours) and less severe. Septic arthritis, on the other hand, is a medical emergency with persistent swelling and fever. For patients who later develop consistent patterns or persistent spinal symptoms, checking criteria for ankylosing spondylitis can help clarify whether a chronic spondyloarthropathy is emerging; see the ankylosing spondylitis criteria for more details.
Is migratory arthritis curable?
Most cases are treatable rather than cured. If a virus sparked the flare, the arthritis often fades once the infection clears. When an autoimmune disease underlies it, ongoing management may be needed.
Quick Comparison Table
| Condition | Joint Pattern | Typical Duration | Key Labs | FirstLine Treatment |
|---|---|---|---|---|
| Migratory Arthritis | Shifts rapidly | Daysweeks | Elevated ESR/CRP, viral serology | NSAIDs steroids |
| Rheumatoid Arthritis | Symmetric, persistent | Monthsyears | RF, antiCCP | DMARDs |
Common Causes & Triggers
Top causes?
Viral infections (think parvovirus B19, hepatitisB/C, even the flu) sit at the top of the list. Autoimmune flares, postCOVID19 inflammation, and certain drug reactions can also set off the jointhopping party.
Can COVID19 trigger it?
Yesstudies are showing a link between COVID19 and a lingering, migratorytype arthritis. One recent review highlighted that up to 10% of recovered patients reported joint pain that moved around for weeks after infection.
Why does it appear in children?
Kids often get viral arthritides from common colds or handfootmouth disease. Occasionally, a juvenile idiopathic arthritis variant mimics migratory patterns, so a pediatric rheumatologists input is key.
How long does it usually last?
For a viral trigger, expect 14weeks of episodes. If an autoimmune condition is at play, the symptoms may linger or recur, demanding a longerterm plan.
RealWorld Example
Take Alex, a 32yearold who recovered from a mild COVID19 case. Two weeks later, his knees, wrists, and ankles started aching one after another. A short course of ibuprofen and a couple of days of lowdose prednisone tamed the flare in five days. By week three, the pain was gone, and hes back to his weekend hikes.
Diagnosing Migratory Arthritis
What tests confirm it?
Doctors start with a thorough historywhen the pain moves, what makes it worse, recent infections, meds, etc. Blood work usually includes a CBC, ESR/CRP, viral panels (like parvovirus), rheumatoid factor, and antiCCP. Imaging is rarely needed unless a specific joint stays swollen.
Differential diagnosis?
When the pain jumps, doctors consider:
- Viral arthritis
- Palindromic rheumatism
- Systemic lupus erythematosus
- Reactive arthritis (postinfection)
- Septic arthritis (must be ruled out quickly)
When to see a rheumatologist?
If swelling persists beyond six weeks, if you develop night pain that wakes you, or if you notice systemic signs like fever, rash, or weight loss, its time to get a specialist involved. For patients with symptoms suggesting axial involvement or chronic back pain, evaluating for ankylosing spondylitis remission goals and longterm monitoring may be appropriate as part of specialist care.
Diagnostic Flowchart
- Symptom onset
- Basic labs (CBC, ESR/CRP)
- Targeted viral or autoimmune panels
- Imaging if needed
- Referral decision.
Treatment Options Balance of Benefits & Risks
Firstline medication?
Nonsteroidal antiinflammatory drugs (NSAIDs) are usually the goto. Ibuprofen 400600mg every 68hours or naproxen 250500mg twice daily can calm pain within a day or two. Remember to take them with food to protect your stomach.
When are steroids needed?
If NSAIDs arent enough, a short burst of oral prednisone (1020mg daily, tapering over 12weeks) can bring rapid relief. Intraarticular steroid shots are an option for stubborn, isolated joints, but theyre not a longterm fix.
Do I need diseasemodifying drugs?
Only if an underlying autoimmune disease is uncovered. In that case, diseasemodifying antirheumatic drugs (DMARDs) like methotrexate or biologics may be introduced, but thats a conversation with a rheumatologist.
Can physiotherapy help?
Absolutely. Gentle rangeofmotion exercises, lowimpact cardio (swimming, walking), and strength training keep joints supple and reduce stiffness. The Mayo Clinic recommends starting with 1015minutes of movement twice a day during a flare.
What about diet?
While no magic food cures the arthritis, an antiinflammatory diet can tip the scales toward healing. Think omega3rich fish, walnuts, turmeric, leafy greens, and plenty of water. Cutting back on processed sugars and saturated fats reduces overall inflammation.
Risks of doing nothing?
Leaving a flare unchecked can lead to chronic joint damage, reduced mobility, and a lower quality of life. It can also mask a more serious condition that needs early treatment.
Treatment Comparison Table
| Treatment | Onset of Relief | Typical Duration | Major Risks | Ideal Patient |
|---|---|---|---|---|
| NSAIDs | 2448h | 2weeks (shortterm) | GI bleed, renal strain | Mildmoderate pain |
| Oral Steroids | 13days | 1month (taper) | Mood swings, glucose rise | Severe flare |
| DMARDs/Biologics | 412weeks | Longterm | Immunosuppression | Chronic autoimmune |
| Physical Therapy | 12weeks | Ongoing | None | All stages |
| Antiinflammatory diet | 24weeks | Ongoing | None | Complementary |
Lifestyle & SelfManagement
Daily routine tweaks?
Sleep is your secret weaponaim for 79hours in a dark, cool room. Stressreduction techniques like deep breathing or brief meditation can lower systemic inflammation. Keep moving, but avoid highimpact activities while a joint is hot.
Helpful supplements?
Fish oil (1g EPA/DHA daily) and vitaminD (if youre low) have modest evidence for easing joint pain. Always chat with your doctor before adding new supplements.
Safe exercise ideas?
Lowimpact options work best: swimming, cycling, yoga, or even a brisk walk. If a joint feels tender, pause that side and focus on the opposite limb to maintain balance.
Tracking progress?
Use a simple symptom diarynote the joint affected, pain level (010), swelling, and any triggers. Over time, patterns emerge, helping you and your doctor finetune treatment.
Sample 7Day SelfCare Plan
- Day12: NSAID with meals, 20minute easy walk, hydrate (2L water).
- Day34: Add fishoil capsule, gentle stretching for 10minutes each morning.
- Day57: Introduce lowimpact yoga, continue diary, assess pain scores.
When to Seek Immediate Help
If you notice any of these red flags, dont wait:
- Sudden joint swelling accompanied by feverpossible septic arthritis.
- Persistent night pain lasting more than two weeks.
- New numbness, tingling, or weakness near the joint.
- Rapid loss of joint function or inability to bear weight.
Call your primary care provider or head to the emergency department right away.
Resources & Trusted References
For deeper dives, the following sources are solid references that you can explore later:
Conclusion
Migratory arthritis can feel like a mystery when the pain jumps from joint to joint, but the good news is that most cases are manageable with the right blend of medication, gentle movement, and an antiinflammatory diet. By understanding common triggersviral infections, postCOVID inflammation, or autoimmune flaresand following a stepbystep treatment plan (starting with NSAIDs, adding shortcourse steroids if needed, and leaning on physiotherapy), you can shrink flaretime from weeks down to days.
Keep a symptom diary, stay in touch with a rheumatologist for persistent or confusing cases, and remember that early, balanced care is the safest road back to your everyday life. Ready to take control? Download our free 7day flaremanagement checklist or schedule a teleconsult with a boardcertified rheumatologist today.
FAQs
What is the first-line treatment for migratory arthritis?
The first-line treatment usually involves NSAIDs like ibuprofen or naproxen, which help reduce pain and inflammation within a couple of days.
When are steroids recommended for migratory arthritis?
Steroids such as oral prednisone may be used if NSAIDs are insufficient, typically as a short course to quickly reduce severe inflammation.
Can physical therapy help with migratory arthritis?
Yes, gentle physical therapy focusing on range-of-motion exercises and low-impact activities helps maintain joint mobility and reduces stiffness.
Is migratory arthritis curable?
Most cases are manageable rather than curable; viral-triggered arthritis often resolves after infection, while autoimmune causes may require ongoing treatment.
When should I see a rheumatologist for migratory arthritis?
Consult a rheumatologist if symptoms persist beyond six weeks, if you experience systemic signs like fever or weight loss, or if joint swelling worsens.