Looking for a quick, clear answer about the EULAR criteria? In a nutshell, theyre a set of internationallyagreed checklists that help doctors decide whether a patient fits a specific rheumatic diseasethink rheumatoid arthritis, lupus, gout, and more. By ticking off the right boxes, clinicians can classify patients consistently, start treatment earlier, and join research studies with confidence.
But its more than a sterile list. These criteria blend science with realworld experience, balancing the benefits of standardisation against the nuances of each patients story. Lets walk through what the EULAR criteria are, why they matter, and how you can use themwithout feeling like youre reading a textbook.
What Are EULAR
Definition and purpose
The European League Against Rheumatism (EULAR) publishes classification criteria for many rheumatic diseases. Theyre designed to identify patients who truly have a condition, so doctors can enrol them in trials, compare outcomes, and apply evidencebased treatments. Think of them as a reliable compass rather than a legal verdictyou still need clinical judgment.
Classification vs. diagnosis
Classification criteria help group patients for research; diagnosis is the doctors final call. A patient might meet the EULAR criteria for RA yet have another overlapping disorder. Thats why clinicians always combine the checklist with a full history, physical exam, labs, and imaging.
Brief history
Since the early 2000s, EULAR has updated criteria for conditions like rheumatoid arthritis (2010), systemic lupus erythematosus (2019), and most recently osteoarthritis (2023). Each revision reflects new evidence, aiming for higher sensitivity (catching more true cases) without sacrificing specificity (avoiding false positives).
Why They Matter
Benefits for clinicians
- Standardised language across Europe and beyond.
- Clear thresholds for starting diseasemodifying therapies.
- Improved eligibility for clinical trials.
- Facilitates communication between specialists and primary care providers.
Benefits for patients
- Earlier, more accurate identification of disease.
- Access to the right treatments faster.
- Confidence that the care plan is based on robust, peerreviewed standards.
Risks and limitations
Because theyre built for classification, these criteria can sometimes miss atypical presentations. Overreliance on a score can delay a nuanced clinical assessment, especially in early disease stages or when comorbidities mask classic signs. Always treat the score as a guide, not a verdict.
Disease Specific
EULAR criteria for RA
The 2010 ACR/EULAR rheumatoid arthritis classification uses a point system that looks at joint involvement, serology (RF and antiCCP), acutephase reactants, and symptom duration. A total score of6 out of10 classifies the patient as having RA.
Quick checklist
- Joint involvement: 05 points.
- Serology: 03 points.
- Acutephase reactants: 01 point.
- Symptom duration: 01 point.
Calculator link
Need a fast way to score? Try the on MDCalc.
EULAR criteria for SLE
For systemic lupus erythematosus, the entry requirement is a positive antinuclear antibody (ANA) at a titre1:80. After that, weighted clinical and immunologic items (e.g., arthritis, renal involvement, antidsDNA) are summed. A total of10 points suggests SLE.
EULAR criteria for APS
Antiphospholipid syndrome (APS) needs at least one clinical event (vascular thrombosis or pregnancy morbidity) plus a positive laboratory test (lupus anticoagulant, anticardiolipin, or 2glycoprotein I antibodies) on two occasions 12weeks apart.
EULAR criteria for scleroderma
Systemic sclerosis classification focuses on skin thickening (proximal to the metacarpophalangeal joints) plus one of the following: specific autoantibodies (anticentromere, antitopoisomerase I), Raynauds phenomenon, or internal organ involvement.
EULAR criteria for gout
The 2022 ACR/EULAR gout criteria combine clinical features (rapidly developing monoarticular arthritis), synovial fluid analysis, and serum urate levels. A weighted algorithm gives a probability; >0.8 classifies gout.
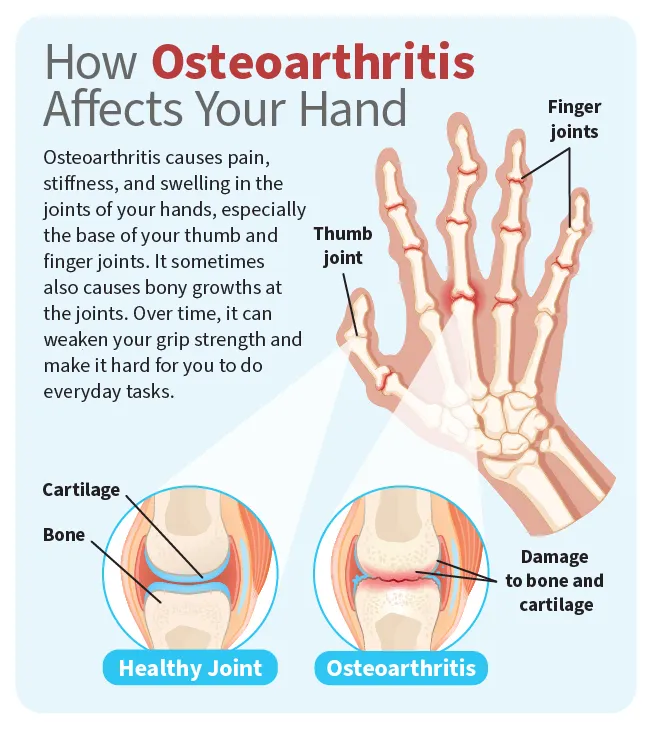
EULAR criteria for osteoarthritis
The 2023 hand osteoarthritis criteria require age50, pain in 2 joints, <30minutes of morning stiffness, and radiographic osteophytes or jointspace narrowing. Scoring 2 points indicates OA.
Other emerging sets
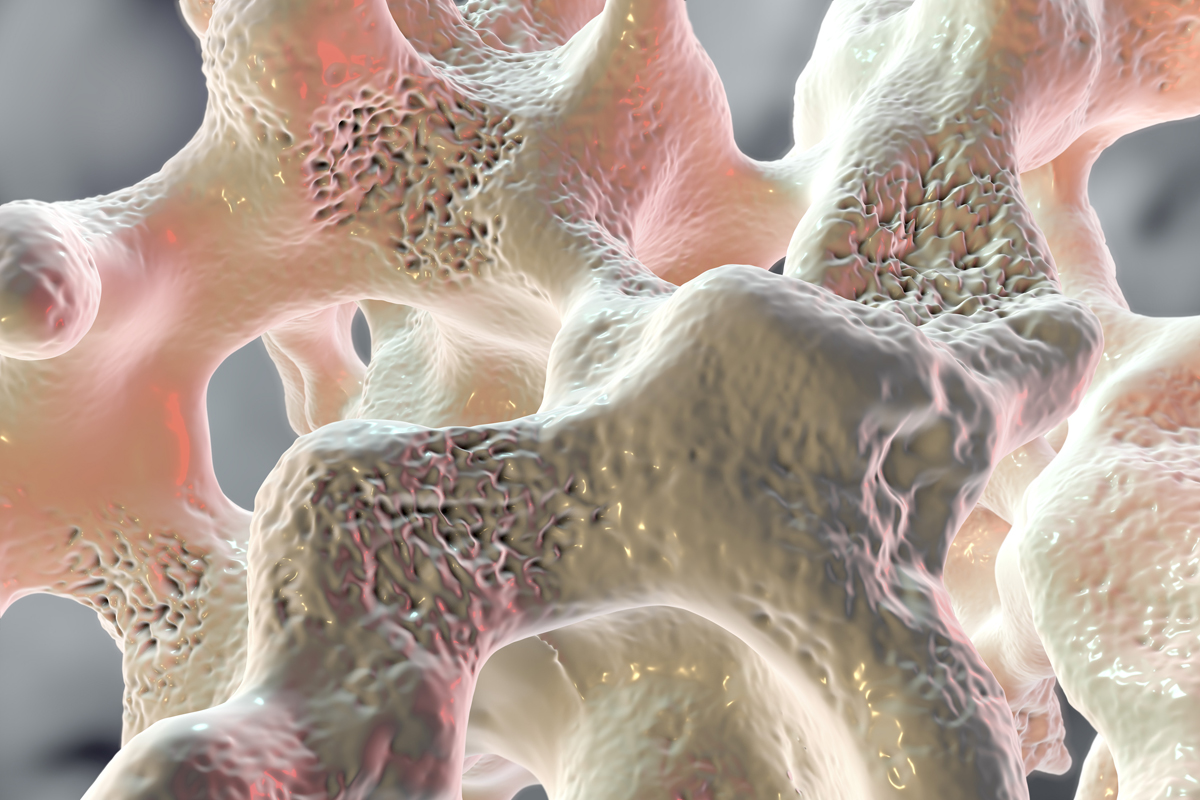
Recent updates (2024) have introduced criteria for chronic nonbacterial osteomyelitis and juvenile idiopathic inflammatory myopathies. They follow the same pattern: clinical domains, lab markers, imaging, and a threshold score.
Applying Criteria
Workflow for everyday practice
- History & physical: Note joint distribution, symptom onset, extraarticular features.
- Laboratory tests: ANA, RF, antiCCP, antiphospholipid antibodies, uric acid, acutephase reactants.
- Imaging: Xray for erosions/osteophytes, ultrasound for synovitis, MRI if needed.
- Scoring: Use the diseasespecific checklist or an online calculator.
- Decision making: If the score meets the threshold, discuss treatment options; if borderline, consider referral or repeat testing.
Tools and apps
Beyond the MDCalc link above, the official EULAR website offers downloadable PDFs of each criteria set. Some mobile apps even let you tick boxes offline and generate a summary report for the clinic.
Interpreting borderline scores
When a patient scores just below the cutoff (e.g., 5 out of 6 for RA), treat it as a gray zone. Reevaluate in 36months, repeat serologies, and consider imaging. Early intervention can still be justified if clinical suspicion is high.
Common Pitfalls
Misusing classification as diagnosis
Remember: a patient may meet the EULAR criteria for RA but still have another inflammatory arthritis. Always confirm with a comprehensive assessment.
Adultchild differences
Children often present differentlyjoint involvement may be less symmetrical, and serology can be negative. Some EULAR criteria have paediatric adaptations (e.g., juvenile SLE), so check the specific version.
Partial fulfillment
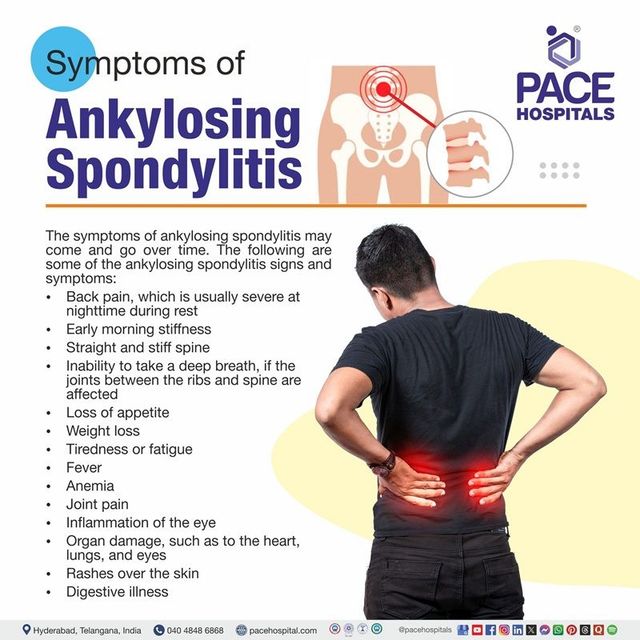
If a patient meets only some items, dont dismiss the possibility outright. Certain early disease phenotypes lack full laboratory positivity; serial monitoring can capture evolution over time. For example, monitoring for ankylosing spondylitis criteria can be particularly helpful when spinal symptoms are subtle.
Latest Updates
20232024 revisions
The most recent updates broadened the hand OA criteria to include ultrasounddetected erosions and introduced a new scoring algorithm for chronic nonbacterial osteomyelitis. These changes aim to improve early detection, especially in primary care settings.
Ongoing validation studies
Multiple international cohorts are currently testing the eular criteria latest versions for sensitivity across diverse ethnic groups. Results are being published in journals like and are worth keeping an eye on.
Future directions
Artificial intelligence may soon assist in autocalculating scores from electronic health records, streamlining the process even further. But until then, the human touchlistening to a patients storyremains irreplaceable.
Trusted Resources
Official EULAR pages
The goto source for the most current criteria is the . It hosts PDFs, updates, and links to supporting literature.
Peerreviewed articles
Key validation studies can be found on PubMed. For instance, the 2020 validation of the RA criteria is described in .
Clinical calculators
Beyond MDCalc, the ACRs own calculator for gout is available . Theyre free, webbased, and regularly updated.
Downloadable checklist
For quick reference, you can download a onepage PDF containing all major EULAR criteria. Its handy to keep on your desk or in the clinics shared folder.
Conclusion
The EULAR criteria are powerful tools that bring consistency, confidence, and clarity to the assessment of rheumatic diseases. By understanding both their strengths and their limits, you can use them to guide treatment decisions while still honouring each patients unique narrative. Whether youre scoring a joint count for RA, checking ANA patterns for SLE, or running a gout calculator, remember that these checklists are alliesnot arbiters. Download the checklist, try the calculators, and share your experiences in the commentsyour insights help us all get better at caring for those who need it most.
FAQs
What are the EULAR criteria?
The EULAR criteria are internationally‑agreed checklists published by the European League Against Rheumatism to help clinicians consistently classify rheumatic diseases for research and treatment decisions.
How do classification criteria differ from a diagnosis?
Classification criteria group patients with similar disease characteristics for studies and guideline use, whereas a diagnosis is the physician’s final clinical judgment after considering the whole patient story.
When should I use the EULAR RA scoring system?
Use the 2010 ACR/EULAR rheumatoid arthritis score when a patient presents with joint pain, possible serology, and acute‑phase reactant changes; a total ≥ 6 out of 10 classifies RA.
What are common pitfalls when applying EULAR criteria?
Typical mistakes include treating the score as a definitive diagnosis, overlooking atypical or early presentations, and applying adult criteria to pediatric patients without the adapted versions.
What are the latest updates to the EULAR criteria?
Recent revisions (2023‑2024) added ultrasound findings to hand osteoarthritis, introduced a scoring algorithm for chronic non‑bacterial osteomyelitis, and refined thresholds for better sensitivity across diverse populations.