Weve all heard the word meningitis and felt that instant knot in our stomach, right? The good news is that when bacterial meningitis shows up, antibiotics are the superhero that can turn a scary situation into a treatable oneif we act fast and choose the right drugs.
In the next few minutes youll get a clear, friendly guide on which antibiotics doctors use, how doses differ for adults and kids, when oral pills are okay, and what the latest say. No jargonfilled paragraphs, just the facts you need to feel informed and confident.
Understanding Meningitis
What Is Bacterial Meningitis?
Think of the meninges as the protective blankets around your brain and spinal cord. When bacteria breach those blankets, they cause inflammation, fever, stiff neck, andif untreatedrapid deterioration. The most common culprits are Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae (though the latter is now rare thanks to vaccination).
Why Antibiotics Matter
Antibiotics are the only weapons that can cross the bloodbrain barrier quickly enough to kill the invading bugs. The phrase time is brain isnt just for strokes; every hour you wait can let the infection spread, increasing the risk of hearing loss, seizures, or even death.
Quick Fact Box
| Statistic | Detail |
|---|---|
| Mortality without treatment | 3050% in adults, higher in infants |
| Typical pathogens | S.pneumoniae, N.meningitidis, H.influenzae |
| Critical window | First 46hours after symptom onset |
FirstLine IV Antibiotics
Cefotaxime
Cefotaxime is a thirdgeneration cephalosporin that reaches high levels in the cerebrospinal fluid (CSF). The usual adult dose is 50mg/kg IV every 6hours, capped at 12g per day. For kids, its 100mg/kg per dose (max 4g) given every 6hours.
Key Points
- Works well against most pneumococci and meningococci.
- Renal dosing adjustments are needed if creatinine clearance falls below 30mL/min.
Ceftriaxone
Ceftriaxone is another goto drug, especially in settings where a oncedaily dosing schedule is preferred. Adults receive a 2gram loading dose, then 2g every 12hours (max 4g/day). Children get 100mg/kg per dose every 12hours, up to the same 4gram ceiling.
Key Points
- Excellent CSF penetration even when meninges are inflamed.
- Can be given intramuscularly if IV access is challengingthough IV remains the gold standard.
When to Add Vancomycin
If theres a risk of drugresistant Streptococcus pneumoniae (often flagged by a local resistance rate>20%), vancomycin joins the party. The typical adult regimen is 15mg/kg IV every 8hours, adjusted to keep trough levels between 1520g/mL.
Monitoring Vancomycin
Because vancomycin can be tough on kidneys and ears, clinicians check serum creatinine and hearing tests after a few days. If the patient shows signs of nephrotoxicity, the dose is trimmed or the drug is swapped for something like linezolid (though linezolid isnt firstline).
Tailoring After Cultures
Once the lab tells us the exact bug and its antibiotic sensitivities, therapy is narrowed. For a penicillinsusceptible S.pneumoniae, highdose penicillinG (4million units IV every 4hours) replaces the broadspectrum agents, minimizing sideeffects.
Pediatric Treatment Regimens
AgeBased Dosing
Kids arent just small adults; their metabolism and CSF dynamics differ. Heres a quick snapshot:
| Age | Cefotaxime | Ceftriaxone | Vancomycin |
|---|---|---|---|
| Neonates (028days) | 150mg/kg q12h | 50mg/kg q12h | 15mg/kg q6h |
| Infants (112months) | 100mg/kg q6h | 100mg/kg q12h | 15mg/kg q8h |
| Children (112years) | 100mg/kg q6h | 100mg/kg q12h | 15mg/kg q8h |
Special Situations
During a meningococcal outbreak, the CDC recommends a singledose intramuscular ceftriaxone for rapid mass prophylaxis, but anyone with confirmed disease still receives full IV therapy.
Case Vignette
Imagine a 4yearold named Maya who arrives with fever, a bulging fontanelle, and a stiff neck. CSF Gram stain shows grampositive diplococci. The team starts cefotaxime 100mg/kg q6h plus vancomycin 15mg/kg q8h. When cultures confirm penicillinsusceptible S.pneumoniae, they switch to highdose penicillin G, and Maya is home in two weeks, hearing intact and smiling.
Oral Antibiotic Options
When Are Pills Okay?
Oral antibiotics arent the first choice for acute bacterial meningitis, but they become valuable when a patient stabilizes after 4872hours of IV therapy, or when the pathogen is known to be fully susceptible (e.g., Neisseria meningitidiswhich is rarely resistant).
Common Oral Agents
- Amoxicillin 90mg/kg/day divided every 8hours for susceptible H.influenzae.
- Levofloxacin 1015mg/kg once daily (max750mg) in adults when fluoroquinolonesensitive organisms are proven.
- Trimethoprimsulfamethoxazole for certain Streptococcus strains, though its used sparingly.
Pros & Cons
Oral therapy is convenient and avoids IV line complications, but the drug must reach therapeutic concentrations in the CSF. Thats why clinicians doublecheck the pathogens susceptibility and ensure the patients lumbar puncture shows a normal or improving CSF profile before switching.
Empiric Treatment Algorithms
Adult Flowchart
If you suspect bacterial meningitis in an adult, the algorithm looks like this:
| Step | What to Give | Why |
|---|---|---|
| 1. Initial | Ceftriaxone+Vancomycin | Broad coverage for common bugs and resistant pneumococci. |
| 2. Adjust | Swap to PenicillinG if culture = penicillinsusceptible S.pneumoniae. | Deescalate to narrowspectrum. |
| 3 | Add Ampicillin for Listeria (50years or immunocompromised) | Specific coverage for a rare but deadly bug. |
Pediatric Flowchart
Kids get a similar backbone, but dosing and the inclusion of ampicillin for Listeria depend on age:
| Age | Empiric Regimen |
|---|---|
| Neonates | Ampicillin+Cefotaxime+Gentamicin |
| Infants>1month | Ceftriaxone+Vancomycin |
| Children | Ceftriaxone+Vancomycin (add Ampicillin if Listeria risk) |
Duration of Therapy
Most bacterial meningitis courses run 1014days. Some conditionslike Listeria or meningitis caused by Enterobacteriaceaemight need 21days. Always follow the for specific pathogen recommendations.
Side Effects & Risks
Common Adverse Events
Even lifesaving antibiotics can cause trouble. Here are the most frequent issues youll hear about:
- Allergic reactions rash, itching, or in rare cases, anaphylaxis.
- Nephrotoxicity especially with vancomycin or highdose cefotaxime; monitor creatinine.
- Ototoxicity highdose vancomycin can affect hearing, so baseline audiograms are wise if treatment extends beyond a week.
- Clostridioides difficile infection a gut upset that can turn serious; probiotic discussion with your doctor may help.
Monitoring Tips
Doctors usually check serum creatinine and liver enzymes every 4872hours. If youre on vancomycin, therapeutic drug monitoring (TDM) ensures the trough stays in the safe range. For children, weightbased dosing adjustments happen quickly as they grow, so pediatric teams redose daily.
What to Do If Something Goes Wrong
If you notice a new rash, worsening kidney function, or ringing in the ears, call your healthcare provider immediately. Often the team can swap to a similarly effective druglike replacing vancomycin with linezolid for resistant Grampositive organismswhile keeping the infection under control.
Helpful Resources
Official Guidelines PDFs
Both the CDC and WHO publish printable PDFs that summarize the latest bacterial meningitis treatment guidelines. Having a copy handy (saved on your phone or printed) makes it easy to discuss specifics with your doctor.
PatientEducation Sites
Trusted sites like the Mayo Clinic and NHS offer plainlanguage explanations of symptoms, when to seek emergency care, and followup steps after hospital discharge. Bookmark them for quick reference.
Clinician Tools
Online dosing calculators (many are free) let you input weight, age, and renal function to get the exact milligram amountno more mental math during a crisis.
Final Takeaways
When bacterial meningitis strikes, the clock ticks, but the right antibiotics can stop the infection in its tracks. For adults, ceftriaxone or cefotaxime plus vancomycin (when resistance is a concern) form the backbone of therapy. Children receive ageadjusted doses, often with ampicillin added for Listeria risk. Oral antibiotics enter the picture only after a solid IV response, and theyre chosen based on precise lab data.
Balancing the lifesaving benefits with potential sideeffects means vigilant monitoring and open communication with your care team. Keep the official meningitis treatment guidelines pdf close, ask questions, and never hesitate to voice concerns about symptoms or drug reactions.
We hope this friendly walkthrough makes the complex world of meningitis treatment antibiotics feel a bit less intimidating. If you or someone you love is navigating this journey, remember youre not alonemedical experts, solid guidelines, and supportive friends are on your side.
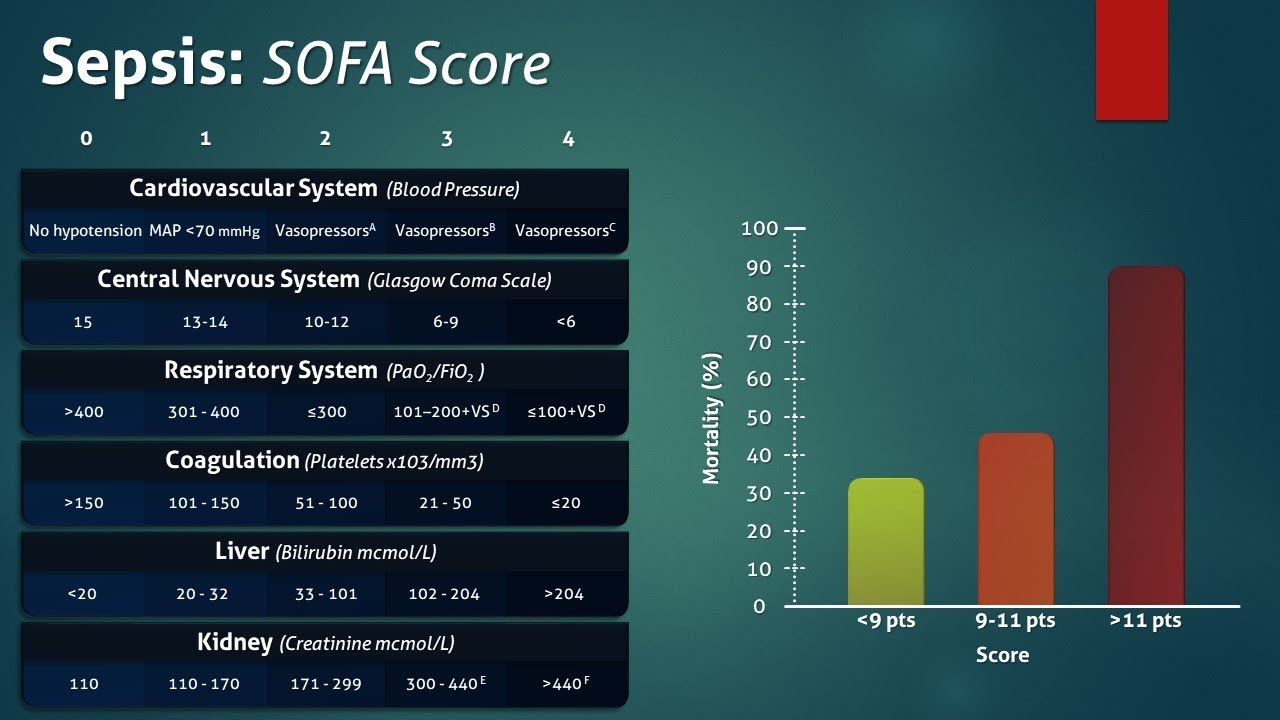
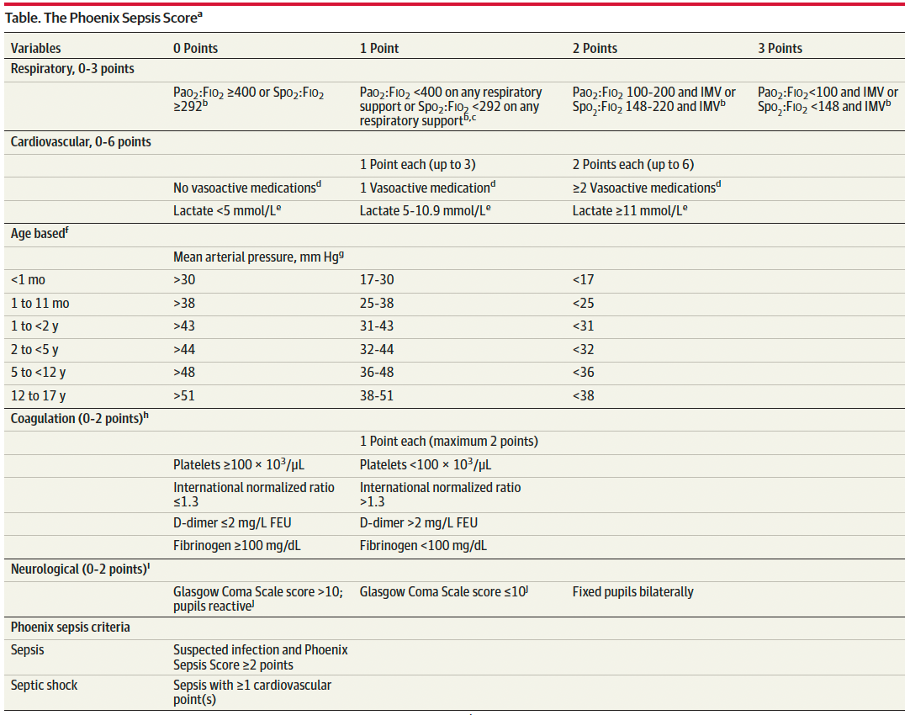
For clinicians assessing organ dysfunction in severe infections, consider referring to updated organ failure assessment resources when determining prognosis and tailoring therapy.
FAQs
What are the first-line antibiotics used to treat bacterial meningitis?
The primary first-line antibiotics for bacterial meningitis are ceftriaxone or cefotaxime, often combined with vancomycin to cover resistant strains. Dosages vary by age and severity.
When is vancomycin added to meningitis treatment?
Vancomycin is added if there is a risk of drug-resistant Streptococcus pneumoniae, typically when local resistance rates exceed 20%, to ensure adequate coverage.
Can bacterial meningitis be treated with oral antibiotics?
Oral antibiotics are generally reserved for after 48–72 hours of intravenous treatment once the patient stabilizes and the pathogen is confirmed susceptible.
What is the typical duration of antibiotic treatment for meningitis?
Treatment typically lasts 10 to 14 days, but may extend to 21 days in cases caused by Listeria or Enterobacteriaceae species.
What are common side effects of meningitis antibiotics?
Common side effects include allergic reactions, nephrotoxicity (especially with vancomycin), ototoxicity, and risk of Clostridioides difficile infection, requiring careful monitoring.