What Is SIRS?
Ever heard someone say, The patient meets SIRS criteria, and wondered what the heck they meant? Youre not alone. In the most straightforward sense, the SIRS score is a bedside tool that flags a possible systemic inflammatory responsethink of it as the bodys alarm system going off. The acronym stands for Systemic Inflammatory Response Syndrome, and it revolves around four vital signs or lab values that, when abnormal, suggest the body is fighting something big.
SIRS Stands For
SIRS = Systemic Inflammatory Response Syndrome. The four pillars are:
- Temperature (fever\xa0or\xa0hypothermia)
- Heart rate (tachycardia)
- Respiratory rate or PaCO (tachypnea or low CO)
- Whitebloodcell count (leukocytosis or leukopenia)
Why It Exists
Back in the early 1990s, clinicians needed a quick way to catch patients who might be spiraling toward sepsis. The SIRS criteria offered a simple, objective checklist that could be done in a few minutesno fancy calculations required. It was especially useful in emergency departments and on hospital wards where time is of the essence.
Is It Still Recommended?
Great question! Even though newer tools like the qSOFA and full SOFA scores have entered the scene, the SIRS score still holds a spot in many protocols. The is updated regularly, and the page notes that many clinicians use SIRS as an earlyscreen before moving on to more complex assessments.
How to Calculate
If youre wondering, Can I just eyeball it? the answer is: you could, but a systematic approach wins every time. Lets walk through each criterion, then well pop in a handy table you can copy onto a sticky note.
Exact Criteria
Each of the four items gets a point when it crosses the threshold. Two or more points = a positive SIRS score. Heres the breakdown:
| Criterion | Positive Threshold |
|---|---|
| Temperature | >38.3C (101F) or <36C (96.8F) |
| Heart Rate | >90 beats per minute |
| Respiratory Rate\xa0/\xa0PaCO | Respiratory rate >20 breaths/min or PaCO <32mmHg |
| WhiteBloodCell Count | >12,000cells/mm, <4,000cells/mm, or >10% immature (band) forms |
Online Calculator
If youre on a computer or phone, the does the math for you in seconds. Plug in the numbers, hit Calculate, and youll see the total score right awayno mental gymnastics needed.
Documentation Tips
When you record each element, be as precise as possible. Note the method of temperature measurement (oral, tympanic, rectal), the time window for heartrate spikes, and whether the whitebloodcell count came from a peripheral draw or a central line. Those little details keep the score reproducible and trustworthy.
SIRS vs Sepsis
Its easy to conflate the two because they share the word infection in many minds. But theyre not synonymous.
Relationship
Think of SIRS as the red flag and sepsis as the danger zone that follows when that red flag is paired with a suspected infection. In other words, a patient who meets SIRS criteria+a clinically plausible infection is considered to have sepsis.
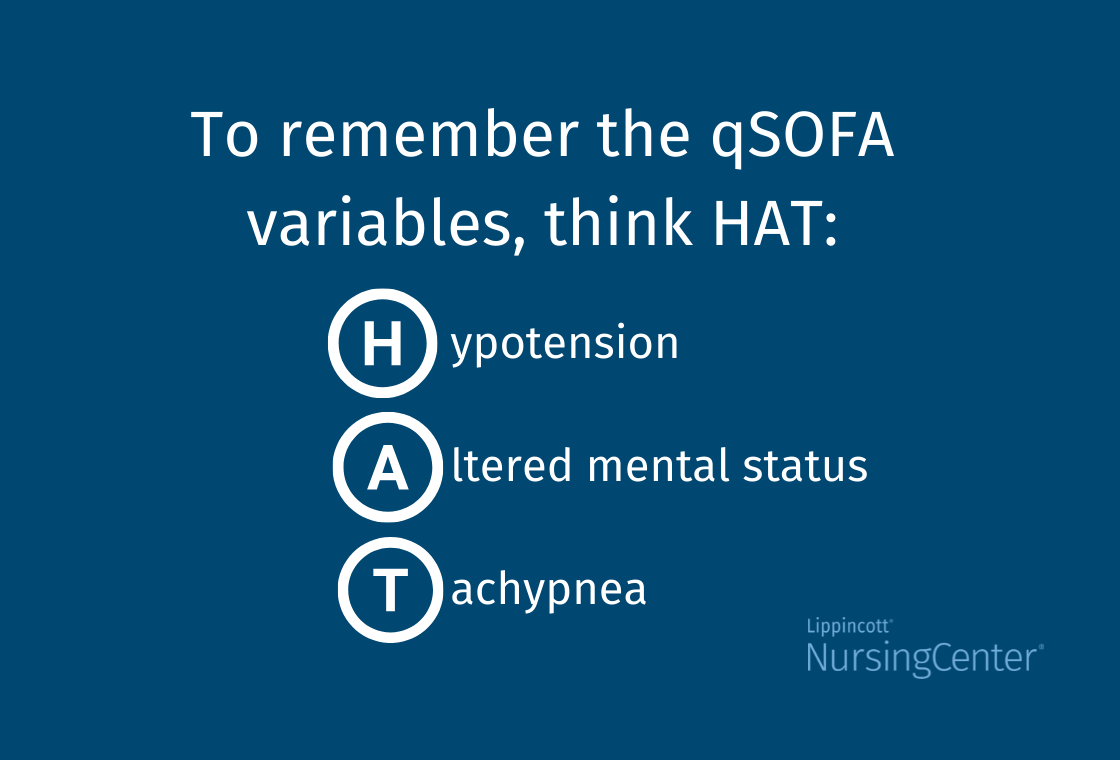
Difference from qSOFA
The qSOFA score zeroes in on mortality risk rather than inflammation. It uses three simple itemsaltered mentation, respiratory rate 22, and systolic blood pressure 100mmHg. While qSOFA is more specific for poor outcomes, SIRS is more sensitive for catching early inflammatory states. A quick comparison:
| Feature | SIRS | qSOFA |
|---|---|---|
| Focus | Systemic inflammation | Mortality risk |
| Sensitivity | High | Moderate |
| Specificity | Lowmoderate | Higher |
| Typical setting | ED, general wards | ED, rapid triage |
When to Switch to SOFA/Septic Shock
After a positive SIRS screen, the next step is to verify infection and then assess organ dysfunction with the full SOFA score. If the SOFA rises by 2 points or more, youre officially in sepsis territory. For septic shock, youll see persistent hypotension despite fluid resuscitation, often needing vasopressors.
When to Use
The SIRS score shines in a few specific situations:
Ideal Settings
- Emergency Department triagequick flag before labs return.
- Postoperative floorsdetect early inflammatory spikes after surgery.
- Trauma baysdistinguish inflammatory response from blood loss.
- Resourcelimited settingsno electronic scoring, just vital signs.
Common Pitfalls
Even the best tools stumble if were not careful. For instance, a patient on steroids might have a blunted fever, or an elderly person may have a normal temperature despite infection. The MDCalc Pearls & Pitfalls note warns against overrelying on temperature alone and reminds us to consider the whole clinical picture.
EHR Integration
Many hospitals have baked SIRS logic into their electronic health records. Epics Sepsis Prediction Model, for example, flags a SIRSpositive patient and nudges the nurse to reassess. Nonetheless, clinicians should still doublecheck the raw numbersautomation is a helper, not a replacement.
Managing Positive Cases
So youve got a SIRS score of 2 or more. What now? The answer is a blend of urgent action and thoughtful followup.
Immediate Action
- Secure the airway, breathing, and circulationABC basics never get old.
- Obtain blood, urine, and possibly wound cultures before starting antibiotics.
- Begin broadspectrum antibiotics in line with your hospitals sepsis bundle.
- Give a 30mL/kg crystalloid fluid bolus if the patient is hypotensive or has signs of poor perfusion.
Escalate to Sepsis Bundle
If infection is suspected, move to the full bundle within the first hour. That includes repeat lactate measurement, vasopressor initiation if MAP stays <65mmHg, and reevaluation of source control.
Special Populations
Older adults, immunocompromised patients, and neonates may not hit the classic thresholds. For example, a bonemarrow transplant recipient could have a normal whitebloodcell count but still be fighting a serious infection. In those cases, clinicians often lower the threshold (e.g., consider SIRS positive with just one abnormal sign plus a high clinical suspicion).
RealWorld Examples
Stories help cement abstract concepts. Here are two quick vignettes that illustrate the powerand the limitsof the SIRS score.
Case 1: PostOp Fever
Maria, a 58yearold who just had a laparoscopic cholecystectomy, spiked a temperature of 38.9C and a heart rate of 102bpm on postoperative day1. Her respiratory rate was 18, and her WBC count was 13,200. Thats a SIRS score of 3. The team ordered cultures, started a short course of antibiotics, and monitored her fluid status. Within 24hours, her vitals normalized, and cultures were negativeturns out it was a transient inflammatory response to the surgery, not sepsis. The early SIRS flag prevented unnecessary escalation while still ensuring vigilance.
Case 2: Trauma OverAlert
Jake, a 27yearold motorcyclist, arrived with multiple fractures. His heart rate was 115, temperature 36.5C, respiratory rate 22, and WBC 8,500. He met three SIRS criteria, but the team recognized the tachycardia and tachypnea were traumarelated, not infectious. They focused on hemorrhage control and analgesia, holding off on antibiotics. Over the next two days, his vitals settled, and no infection emerged. This vignette highlights the importance of contextSIRS can be a red herring when trauma dominates the picture.
Trusted Clinical Sources
When you want to dive deeper or cite the data, these resources are the gold standard:
These citations give you a solid, evidencebacked foundation. Feel free to click through and explore the original researchtheres nothing like reading the source material yourself.
Conclusion
Wrapping it all up, the SIRS score is a fast, lowtech safety net that helps clinicians spot an early inflammatory response before things get out of hand. Its not perfectthere are false positives, especially in trauma or postoperative settingsbut when paired with clinical judgment, infection suspicion, and newer tools like qSOFA or SOFA, it becomes a powerful ally. Remember to use a calculator (or the handy table above), keep an eye on common pitfalls, and act swiftly when the score lights up. By balancing the benefits (early detection) with the risks (overdiagnosis), youll provide safer, more focused care.
Whats your experience with the SIRS score? Have you seen a case where it saved a lifeor where it led you down the wrong path? Share your thoughts in the comments, and lets keep the conversation going. If youre looking for a quick reference, download the printable and keep it on your workbench. Together we can make sure the alarm stays helpful, not noisy.
FAQs
What is the SIRS score used for?
The SIRS score is a quick bedside tool used to detect systemic inflammatory response by assessing vital signs and labs, helping to identify patients at risk of sepsis early.
How is the SIRS score calculated?
It assigns one point for each of four criteria met: abnormal temperature (>38.3°C or <36°C), heart rate >90 bpm, respiratory rate >20 breaths/min or low PaCO₂ (<32 mm Hg), and abnormal white blood cell count (>12,000, <4,000, or >10% bands). Two or more points indicate a positive SIRS score.
What is the difference between SIRS and sepsis?
SIRS indicates systemic inflammation and is a red flag, while sepsis is diagnosed when SIRS criteria occur in the presence of a suspected infection plus organ dysfunction.
When should the SIRS score be used clinically?
The SIRS score is ideal for early screening in emergency departments, post-operative units, trauma bays, and resource-limited settings, facilitating prompt recognition of inflammatory states.
How does the SIRS score compare to qSOFA?
SIRS is more sensitive for detecting early inflammation but less specific, while qSOFA focuses on predicting mortality risk with fewer criteria and higher specificity.