Hey there! If youve ever wondered how doctors quickly decide whether an infection has turned into a lifethreatening emergency, youre in the right place. In a nutshell, sepsis scoring is a set of simple bedside checks that turn messy vital signs and lab numbers into a clear risk grade. This grade tells the care team if they need to start antibiotics right away, move a patient to the ICU, or keep a close eye on them. Lets dive in together and see how you can understandand maybe even explainthese scores without a PhD.
Quick Answer Summary
What is sepsis scoring? Its a quick, evidencebased way to turn a patients vitals, lab results, and organfunction data into a single number that indicates how severe the sepsis might be.
When should you use it? The moment you suspect an infectionwhether youre in the emergency department, on a regular ward, or watching a patient in the ICU. Different tools (SIRS, qSOFA, SOFA, etc.) work best in different settings, and well walk through which one fits where.
Core Scoring Systems
SIRS Criteria
The Systemic Inflammatory Response Syndrome (SIRS) is the oldschool starter. You need at least two of these four points:
- Body temperature<36C or>38C
- Heart rate>90beats/min
- Respiratory rate>20breaths/min or PaCO<32mmHg
- Whitebloodcell count<4,000or>12,000cells/L
Because its simple, SIRS still shows up on many , especially in lowresource settings where labs are limited.
qSOFA Score
The quick SOFA (qSOFA) is a threeitem bedside tool that shines in the ED:
- Respiratory rate22/min
- Systolic blood pressure100mmHg
- Altered mental status (Glasgow13)
If you score 2or more, the patient is at high risk of poor outcomes. Its a neat bridge between the very simple SIRS and the full SOFA.
Full SOFA Score
SOFA (Sequential Organ Failure Assessment) looks at six organ systems. Each gets a score from 0 to 4, giving a total from 0 to 24. Below is a handy sepsis score chart you can print out.
| Organ System | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|---|
| Respiration (PaO/FiO) | >400 | 400 | 300 | 200 | 100 |
| Coagulation (Platelets,10/L) | >150 | 150 | 100 | 50 | 20 |
| Liver (Bilirubin,mg/dL) | <1.2 | 1.21.9 | 2.05.9 | 6.011.9 | >12.0 |
| Cardiovascular | MAP70mmHg | MAP<70 | Dopamine5g/kg/min | Dobutamineany dose | Vasopressors |
| Central Nervous System (GCS) | 15 | 1314 | 1012 | 69 | <6 |
| Renal (Creatinine,mg/dL) | <1.2 | 1.21.9 | 2.03.4 | 3.54.9 | >5.0 or urine<200mL/day |
In the ICU, clinicians often track SOFA daily; a rise of 2 points predicts a markedly higher mortality risk.
Other Scoring Tools
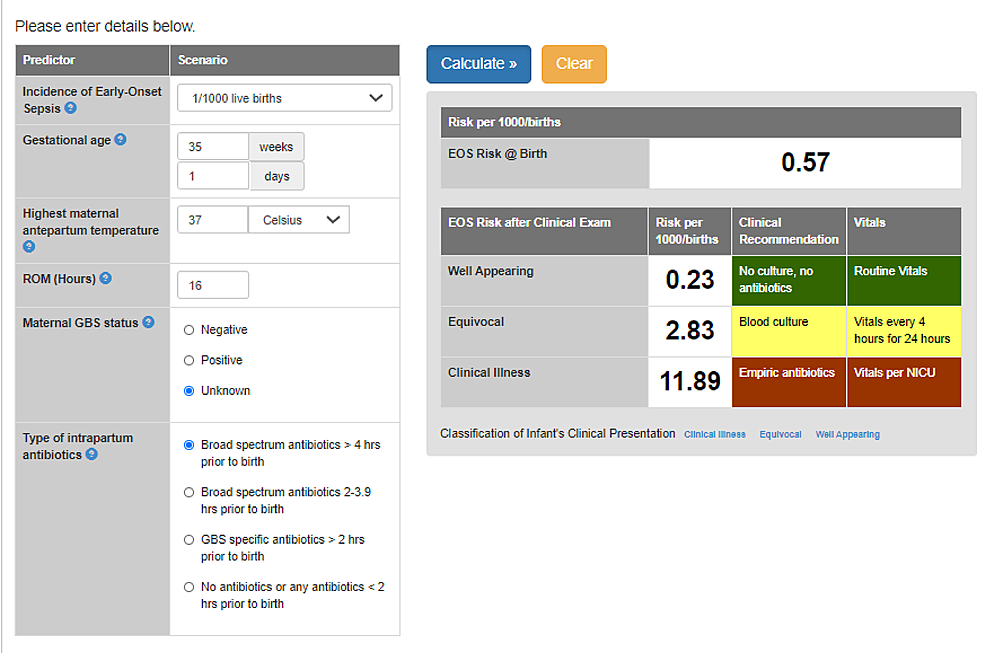
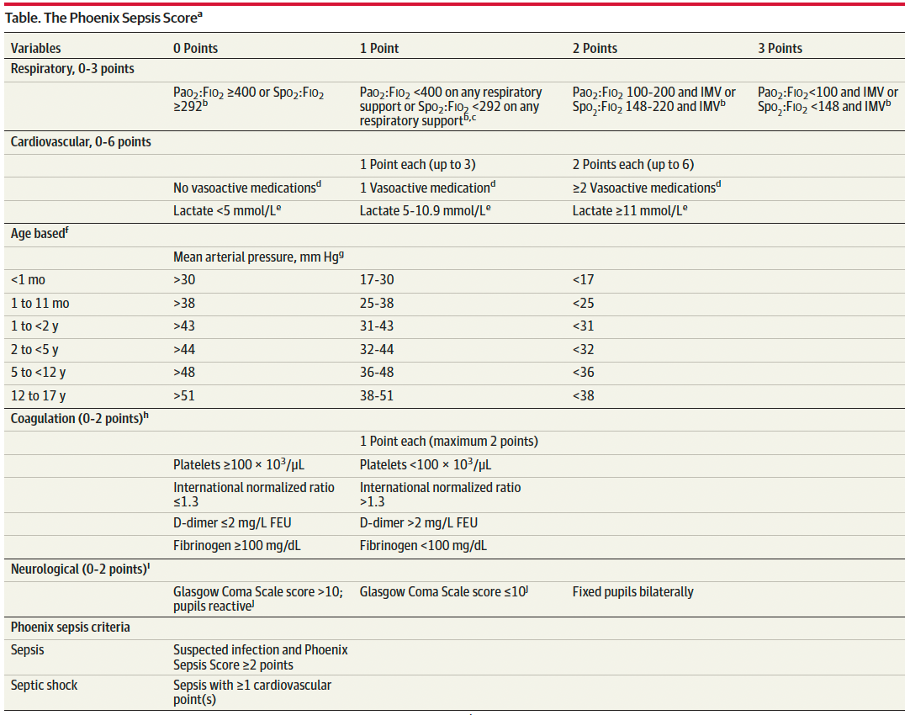
Beyond the big three, there are specialty tools like the MEDS score for ED mortality, the pediatric PELOD2, and even the neonatal used for newborns. Theyre handy when you need a finertuned picture for specific age groups.
Sepsis3 Criteria (2024 Update)
The most recent consensus from the Society of Critical Care Medicine (SCCM) still hinges on qSOFA and full SOFA, but adds clearer guidance on lactate thresholds and the need for rapid antimicrobial therapy. This is what we refer to when we say sepsis3 criteria.
Choosing the Right Score
Emergency Department
In the bustling ER, time is everything. Start with qSOFA plus a quick lactate check. If qSOFA2 or lactate2mmol/L, jump to the full SOFA and start broadspectrum antibiotics immediately.
Intensive Care Unit
Inside the ICU, you already have labs at hand, so the SOFA score becomes your daily dashboard. Track the total and look for a2 rise as a red flag for worsening organ dysfunction.
General Ward / LowResource Settings
Here the SIRS criteria or a printable sepsis score chart often suffices. Its quick, requires only vitals and a basic blood count, and still catches many patients who need escalation.
Pediatrics & Neonates
Kids arent just small adults; they have unique physiology. Use the neonatal for newborns, and the pediatric sepsis criteria (ageadjusted qSOFA) for older children.
Telemedicine & Remote Monitoring
When youre consulting over a video call, the qSOFA or an online MDCalc tool can be a lifesaver. Just be sure the data you receive (BP, RR, mental status) is accurate, and document everything for medicolegal safety.
Calculator StepbyStep
Access the Tool
Open your browser and head to a reputable site like . Search sepsis calculator and youll see options for SIRS, qSOFA, and full SOFA.
Enter Patient Data
Gather these pieces of info:
- Temperature, heart rate, respiratory rate, blood pressure
- Whitebloodcell count (if available)
- PaO/FiO ratio, platelet count, bilirubin, creatinine
- Glasgow Coma Scale (or mental status note)
- Lactate level (optional but recommended)
Read the Output
The calculator will spit out a number. For qSOFA, 2or more means high risk. For SOFA, a total2 indicates organ dysfunction, and a rise of 2 points over 24hours signals a poor prognosis.
Document the Score
Paste the result into the patients SOAP note:
Subjective: Patient with suspected pneumonia.Objective: qSOFA=2 (RR24, SBP95, AMSyes).Assessment: Highrisk sepsis.Plan: Broadspectrum antibiotics, ICU consult.
ReScore Over Time
In the ED, repeat qSOFA every 24hours until youre sure the patient is stable. In the ICU, run a full SOFA daily and chart the trend. Visual graphs help teams see whether the patient is improving or slipping.
Benefits and Risks
Clinical Benefits
When applied correctly, sepsis scoring shortens the time to antibioticsa key factor in survival. It also gives a common language for nurses, physicians, and families to discuss the seriousness of the illness.
Potential Pitfalls
Scores are not magic. They can miss atypical presentations (e.g., immunocompromised patients who dont mount a fever) or flag noninfectious inflammation (like postsurgical patients). Overreliance may lead to unnecessary antibiotics, which fuels resistance.
Evidence Snapshot
Recent systematic reviews (see a study in Critical Care Medicine) show that each point increase in SOFA adds roughly a 12% rise in mortality. Meanwhile, qSOFAs specificity is higher than SIRS but its sensitivity is modestmeaning youll miss some cases if you use it alone.
Mitigating the Risks
Always pair the number with your clinical gut feeling. Ask yourself:
- Does the patient look sick beyond the score?
- Are there other explanations for abnormal labs?
- Is the trend upward, downward, or flat?
That balance turns a cold number into a compassionate decision.
RealWorld Case Examples
Case 1 ED Presentation
Jane, a 62yearold with a cough, arrives with RR28, SBP95, and is a little confused. Her qSOFA is 2. The team runs a quick lactate (2.5mmol/L) and jumps to a full SOFA, which comes back at 8. Within an hour, broadspectrum antibiotics start, and shes transferred to the ICU for closer monitoring. She recovers fully.
Case 2 ICU Progression
Mike, a 48yearold with abdominal sepsis, had an admission SOFA of 6. Over the next 48hours, his score rose to 12, driven by worsening kidney function (creatinine4.2mg/dL) and declining respiratory ratio. The team escalated vasopressor support and consulted nephrology. Although he survived, the steep SOFA rise highlighted the need for aggressive early intervention.
Expert Insight
Dr. Elena Ramos, an ICU director at a major teaching hospital, notes: Scores give us a snapshot, but the story is in the trajectory. A flat SOFA for three days is reassuring; a jump of two points overnight is an alarm bell.
Key Authoritative Resources
When you want to dive deeper, check out these trusted sources:
- The 2024 SCCM Sepsis3 consensus statement (available on the SCCM website)
- Peerreviewed review Scoring systems for the characterization of sepsis (PMCID5233540)
- Clinical guideline Early Recognition of Sepsis in the Emergency Department (published in Critical Care Medicine)
Final Takeaway Summary
Sepsis scoring is a powerful, evidencebased shortcut that helps clinicians turn a jumble of numbers into a clear picture of risk. By picking the right tool for your settingwhether its SIRS on a busy ward, qSOFA in the ED, or the full SOFA in the ICUyou can catch severe sepsis early, start lifesaving treatment, and keep patients safe. Remember, the score is a guide, not a verdict; pair it with your clinical intuition, watch the trends, and youll be part of the team that turns scary numbers into hopeful outcomes.
Whats your experience with sepsis scoring? Have you found a particular tool more helpful in your practice or bedside care? Share your thoughts belowlets keep the conversation going and help each other stay sharp.
FAQs
What is the difference between SIRS and qSOFA for sepsis scoring?
SIRS uses temperature, heart rate, respiratory rate, and white‑blood‑cell count, requiring two abnormal values. qSOFA is a three‑item bedside tool (respiratory rate, blood pressure, mental status) that predicts poor outcomes and is faster in the ED.
When should the full SOFA score be calculated?
The full SOFA is used in the ICU or whenever comprehensive lab data are available. It assesses six organ systems and is repeated daily; a rise of ≥ 2 points signals worsening organ dysfunction.
Can sepsis scoring be used in low‑resource settings?
Yes. In environments without extensive labs, the SIRS criteria or a printable sepsis score chart (vitals + basic blood count) provides a practical way to identify patients who need escalation.
How does lactate level fit into sepsis scoring?
Lactate isn’t part of the scoring numbers but is an important adjunct. A lactate ≥ 2 mmol/L combined with a qSOFA ≥ 2 or a rising SOFA strengthens the suspicion of sepsis and prompts immediate treatment.
Is sepsis scoring reliable for immunocompromised patients?
Scoring tools may miss atypical presentations (e.g., no fever). Clinicians should combine scores with clinical judgment, looking out for subtle signs and considering a lower threshold for treatment.