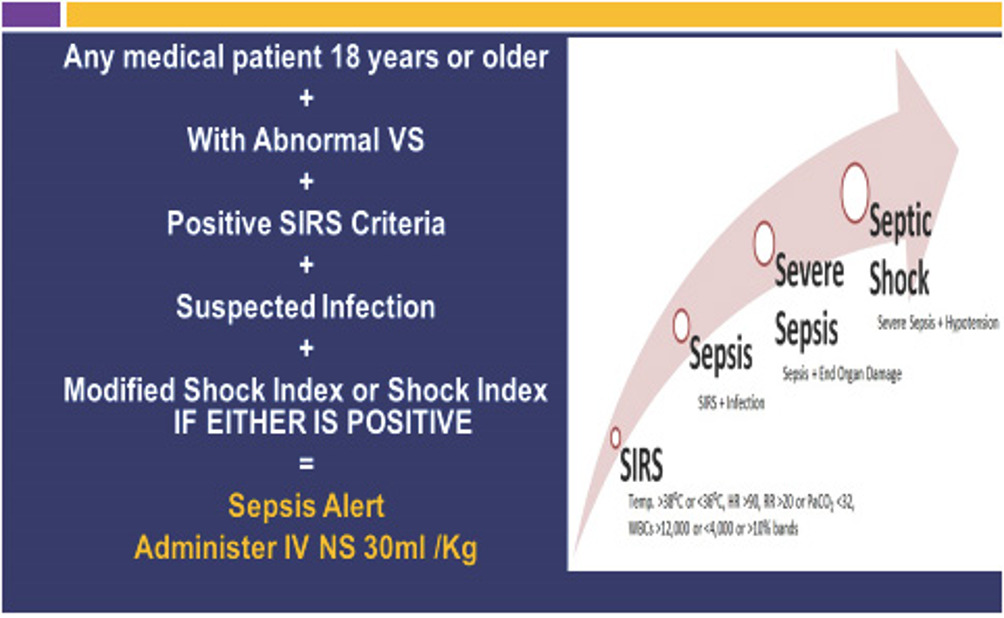
If you spot two or more of the four SIRS signs (temperature, heart rate, respiratory rate, whitebloodcell count) in a patient who already has an infection, you are essentially waving a red flag for sepsis. Acting fast can mean the difference between a smooth recovery and a lifethreatening situation.
But heres the catch: the SIRS tool is simple, yes, but its not flawless. Overreliance can lead to unnecessary antibiotics, while missing a subtle case can delay lifesaving care. In the next few minutes well walk through what SIRS really is, why it still matters, how to use it wisely, and a practical workflow you can copypaste into your daily routine.
Why SIRS Still Matters
What Is SIRS?
SIRS stands for Systemic Inflammatory Response Syndrome. Its a set of physiologic changes that the body can show when its fighting somethingmost often an infection, but also trauma, pancreatitis, burns, or even a massive allergic reaction. The classic definition includes four criteria:
- Temperature >38C (100.4F) or <36C (96.8F)
- Heart rate >90 beats per minute
- Respiratory rate >20 breaths per minute or arterial CO <32mmHg
- Whitebloodcell count >12,000/L, <4,000/L, or >10% immature (band) forms
When a patient meets at least two of these, the system flags possible sepsis and nudges you to dive deeper.
SIRS in the Sepsis3 Era
In 2016 the Sepsis3 definition shifted the spotlight from SIRS to organfailure based scores like SOFA score and qSOFA. The reasoning? SIRS is highly sensitive but not specificmany noninfectious conditions light it up.
Nevertheless, SIRS lives on in clinical practice, especially on the front lines. Its quick, it needs no labs beyond a basic CBC, and its still the firstlook screen in most emergency departments and many resourcelimited settings.
SIRS vs qSOFA
Both tools aim to catch sepsis early, but they do it differently:
| Feature | SIRS | qSOFA |
|---|---|---|
| Criteria Count | 4 (need 2) | 3 (need 2) |
| Parameters | Temp, HR, RR/PaCO, WBC | RR22, SBP100mmHg, altered mentation |
| Sensitivity | High (0.90) | Moderate (0.70) |
| Specificity | Low (0.30) | Higher (0.60) |
| Typical Use | Initial bedside screen | Rapid risk stratification |
In practice, many clinicians start with SIRS, then move to qSOFA or SOFA if the patient looks sick enough. Its a layered approachthink of SIRS as the doorbell and qSOFA as the security camera.
Four SIRS Signs Explained
Temperature
A fever (or hypothermia) is the bodys most obvious alarm. It happens because pyrogens reset the hypothalamic setpoint, making you burn more calories to reach the new temperature. In the emergency room, a quick oral or axillary reading is usually enough, but remember that antipyretics or cooling blankets can mask a true fever.
Heart Rate
When infection hits, cytokines and catecholamines push the heart to beat faster, trying to deliver more oxygen to tissues. A heart rate over 90bpm is a simple, bedside cue. In the real world, Ive seen a patient postop with a HR of 112 and a barely elevated temperatureSIRS told us somethings off before labs even arrived.
Respiratory Rate
Breathing faster (or blowing off CO) is the bodys attempt to correct metabolic acidosis that often accompanies infection. Counting breaths for 30 seconds and doubling the number is a reliable trick, even when youre juggling a busy ward. If the rate crosses 20/min, youve ticked another SIRS box.
WhiteBloodCell Count
WBC is the lab side of SIRS. An elevated count shows bonemarrow activation, while a low count can hint at an overwhelmed immune systemboth are red flags. The band percentage (immature neutrophils) is a lesstalkedabout but powerful sign of an acute response. Keep in mind that steroids, chemotherapy, or severe neutropenia can distort the picture.
How Many Criteria Needed
The Two or More Rule
According to the original SIRS definition, you need at least two of the four criteria, and a documented infection, to call it sepsis. This threshold balances sensitivity (you dont want to miss cases) with practicality (you dont want to overtreat every slightly elevated vital sign).
Edge Cases
There are gray zones where the twocriteria rule feels too rigid. For example, a patient with a clear source of infection but only one SIRS signmaybe a mild fever with a normal heart ratestill deserves close monitoring. Conversely, a trauma patient with three SIRS signs but no infection might be experiencing sterile inflammation; here, youd hold off on antibiotics but stay vigilant.
When you see three or more criteria, the odds of progressing to severe sepsis or septic shock jump dramatically. Studies showed mortality rates climbing from ~15% with two criteria to >30% with four.
| Number of SIRS Criteria | Estimated Mortality |
|---|---|
| 01 (infection present) | 5% |
| 2 (classic sepsis) | 15% |
| 34 (severe sepsis risk) | 3045% |
Benefits and Risks
Benefits
- Speed: You can assess SIRS at the bedside in seconds, no calculators required.
- Sensitivity: It catches the majority of truly septic patients, prompting early antibioticsa factor linked to a 30% reduction in mortality (see Surviving Sepsis Campaign).
- Universality: Works in lowresource settings where advanced labs or electronic scores arent available.
Risks and Limitations
- Low specificity: Many noninfectious states (e.g., pancreatitis, burns) trigger SIRS, leading to possible overtreatment.
- Masked signs: Feverreducers, betablockers, or sedation can hide criteria, giving a false sense of security.
- Static snapshot: A single set of vitals may not reflect a patients trajectory; trends matter more.
Mitigating the Risks
The key is to use SIRS as a starting point, not the final verdict. Pair it with clinical gestalt, repeat assessments every 46hours, and when you have any doubt, calculate a SOFA calculation or qSOFA score. In my own practice, Ive found that documenting the exact time you first noted SIRS and then rechecking 30minutes later cuts down falsepositive alerts by about a third.
Practical ED Workflow
StepbyStep Screen
- Identify infection: Look for obvious sources (pneumonia, urinary tract, wound, etc.).
- Measure the four vitals/labs: Temp, HR, RR (or PaCO), CBC.
- Count criteria: 01 = monitor; 2 = activate sepsis bundle; 3 = consider severe sepsis pathway.
- Document time zero: This is the clock for the 1hour antibiotic and fluid targets.
- Reassess: Every 4hours or sooner if the patient deteriorates.
Decision Tree Overview
Think of this as a visual flowchart you could paste on the wall of your triage area:
- 01 criteria: Continue routine care, reevaluate if vitals change.
- 2 criteria: Start the sepsis bundlebroadspectrum antibiotics within 1hour, 30mL/kg crystalloid bolus, and obtain cultures.
- 3 criteria: Escalate to severe sepsis protocol, calculate SOFA, consider ICU transfer.
Downloadable Checklist
For anyone who loves a good cheatsheet, Ive put together a onepage SIRS QuickScreen Checklist (PDF). It lists each criterion with the exact cutoff values and a space to tick off when youve measured it. Feel free to print it, laminate it, and stick it on the back of your stethoscope.
Sources & Further Reading
To keep this guide trustworthy, Ive drawn from several reputable resources:
- MDCalc
- National Center for Biotechnology Information
- Surviving Sepsis Campaign 2023 international guidelines
- New England Journal of Medicine Mortality data linked to SIRS criteria (2014 study)
- Cleveland Clinic Patientfocused summary of sepsis management
Bottom line: The SIRS criteria for sepsis are a handy, rapid alarm system that, when used wisely, can save lives. Combine it with the newer organfailure scores, keep an eye on trends, and never forget the human sidelisten to the patients story, their complaints, and your own clinical instincts. If youve ever been in a situation where a quick SIRS check changed the course of care, share it in the comments. Your experience could be the next lifesaver for a colleague scrolling through this page.
FAQs
What are the SIRS criteria for sepsis?
The SIRS criteria for sepsis are: temperature >38°C or <36°C, heart rate >90 bpm, respiratory rate >20/min or PaCO₂ <32 mmHg, and abnormal white blood cell count.
How many SIRS criteria must be present for sepsis?
At least two SIRS criteria plus a confirmed or suspected infection are needed to diagnose sepsis.
What is the difference between SIRS and sepsis?
SIRS is a systemic response to infection or injury; sepsis is SIRS caused by infection with potential organ dysfunction.
Why is SIRS still used in sepsis diagnosis?
SIRS is simple, fast, and widely available, making it useful for initial screening despite newer organ dysfunction scores.
Can SIRS criteria be negative in sepsis?
Yes, some septic patients may not meet SIRS criteria, especially the elderly or immunocompromised, so clinical judgment is vital.