What Is Preterm Labor?
Preterm labor kicks in any time before 37weeks of pregnancy. Its basically the uterus starting to contract and the cervix beginning to thin out earlier than expected. The goal of delaying it isnt to stop it forever (that would be a miracle), but to pause it just long enough to deliver crucial care to the baby and to the mother.
Why Do We Try to Delay?
Think of a preterm birth like trying to catch a flight thats about to leave. Every minute you buy before the doors close allows you to finish your packing, get a passport stamped, or call a friend for a lift. In the medical world, those minutes translate into:
- Administration of corticosteroids to mature the babys lungs.
- Magnesium sulfate for neuroprotection.
- Arranging transport to a hospital with a levelIII NICU.
- Giving the mother a chance to rest and gather support.
RealWorld Example
One mom on a parenting forum shared that she was at 32weeks when contractions started. After a quick hospital visit, doctors gave her a tocolytic and steroids. She bought three extra days before delivery, and those days made a huge difference in her babys weight and breathing ability.
Typical Timeframes
Standard Medical Delays
Most tocolytic drugs such as nifedipine or indomethacin are designed to halt contractions for about 48hours. This window matches the time needed for a full steroid course, and its supported by guidelines from the .
Longer Delays
When Magnesium sulfate is added, especially for babies under 34weeks, the delay can stretch to 57days. The notes that combination therapy sometimes extends the pause enough for a second steroid dose or for transport.
QuickScan Comparison Table
| Gestational Age | Common Tocolytic | Typical Max Delay | What the Delay Enables |
|---|---|---|---|
| <24weeks | Nifedipine, MgSO | 2448hrs | Steroids, safe transport |
| 2434weeks | Indomethacin, MgSO | 48hrs7days | Full steroid course, NICU prep |
| >34weeks | Nifedipine, Ritodrine | 48hrs3days | Birth planning, maternal recovery |
Factors That Influence Delay
Gestational Age Matters
At 32weeks, doctors are more aggressive with tocolytics because the baby still has a solid chance to gain weight. By 34weeks, the benefits start to taper many clinicians focus more on delivery planning than on trying to hold back contractions.
Underlying Cause
Infections, cervical insufficiency, or placental problems can blunt the effectiveness of medication. If the trigger is an infection, antibiotics take priority over tocolysis.
Maternal Health
High blood pressure, diabetes, or cardiac issues might limit which drugs are safe. Your OBGYN will weigh the risks and benefits before prescribing.
Drug Choice & Dosing
Nifedipine is often firstline because its oral and relatively gentle. Indomethacin is great before 32weeks but can affect fetal kidneys if used later. Magnesium sulfate doubles as a neuroprotective agent and a tocolytic, especially useful under 34weeks.
Expert Insight Prompt
Consider adding a quote from a maternalfetal medicine specialist explaining why tocolytics are generally discontinued after 34weeks the benefitrisk curve shifts dramatically.
Medical Interventions That Can Delay Labor
Tocolytics Overview
Tocolytics are a fancy word for contractionstoppers. They work by relaxing uterine muscles or blocking the chemicals that trigger contractions. The most common ones and their typical windows are:
- Nifedipine oral calcium channel blocker, 48hour window.
- Indomethacin prostaglandin inhibitor, best before 32weeks.
- Magnesium sulfate neuroprotective, can extend delay to a week.
All of these are discussed in detail by the and the .
Magnesium Sulfate
Beyond buying time, magnesium protects the babys brain from bleeding. That double benefit makes it a goto for many providers when the baby is under 34weeks.
When to Transfer
If youre at a community hospital and the baby is under 32weeks, a transfer to a levelIII NICU is usually recommended. The decision hinges on distance, transport time, and whether the hospital can administer steroids and magnesium. If you want more information on premature labor symptoms, review the signs that prompt rapid transfer decisions.
StepbyStep Flowchart (text version)
1. Diagnosis of preterm labor 2. Administer tocolytic 3. Give corticosteroids (24hrs) 4. Arrange NICU transfer if<34weeks 5. Monitor uterine activity.
How Long Can Labor Be Delayed at Specific Weeks?
At 32Weeks
At this sweet spot, doctors often achieve a 48hour pause with nifedipine, then add magnesium to stretch the delay up to 57days. Those extra days can translate into a 150gram weight gain for the baby, which is huge for lung development.
At 34Weeks
Most clinicians aim for a 48hour to 3day window. After 34weeks, the risk of medication side effects outweighs the modest fetal growth benefit, so the focus shifts to preparing for delivery rather than trying to stop labor.
At 20Weeks
Early preterm labor is rare and tricky. Tocolysis is limited, and the priority is close monitoring. The goal is often to prevent further progression rather than to achieve a full term birth.
MiniFAQ (embedded)
Can preterm labor be stopped at 20 weeks? Its extremely challenging; interventions mainly aim to buy a few hours for monitoring and to plan for possible later interventions.
Recognizing Early Signs
Key Symptoms
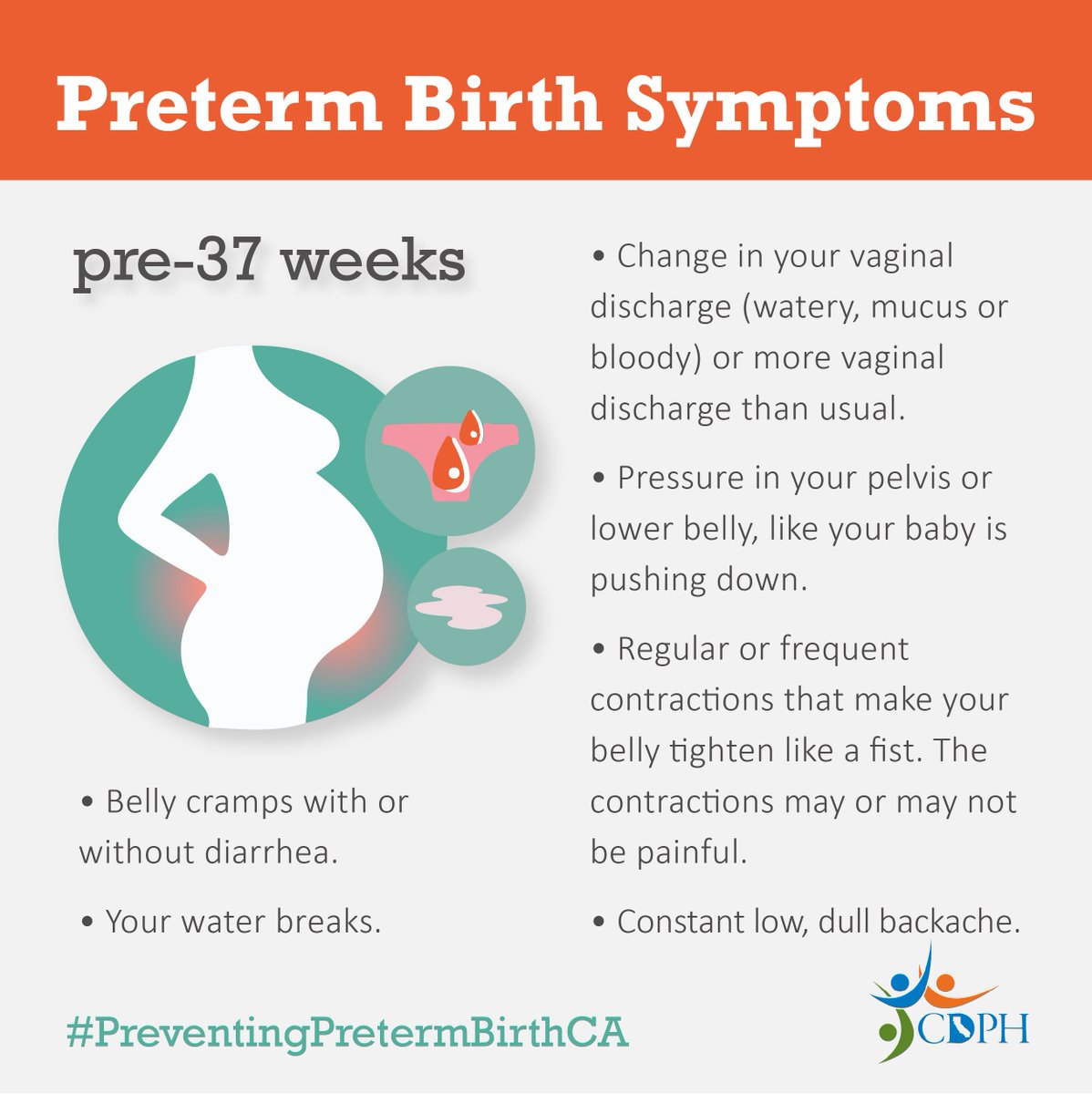
Knowing the warning signs can save precious time. Watch for:
- Regular contractions (every 510minutes) lasting at least 30seconds.
- Pelvic pressure or lowback pain that doesnt go away.
- Changes in vaginal discharge watery, mucusfilled, or tinged with blood.
- Feeling like the baby is dropping suddenly.
False vs. True Labor
False labor (BraxtonHicks) feels like irregular, painless tightening. True preterm labor is rhythmic, progressive, and often accompanied by other symptoms.
Checklist (downloadable PDF idea)
Consider offering a printable Preterm Labor Symptom Checklist that moms can keep by the bedside.
Lifestyle & Positioning Tips
Sleeping Position
Most obstetricians recommend sleeping on your left side. This improves uterine blood flow and may reduce contraction frequency. The highlights leftside sleep as a simple, lowrisk strategy.
Activity Modification
While complete bed rest isnt recommended, limiting prolonged standing, heavy lifting, and highimpact exercise can help ease uterine irritability.
Hydration & Nutrition
Staying wellhydrated (aim for at least 8 glasses of water daily) and eating a balanced diet rich in protein, iron, and folate supports both mother and baby.
Stress Reduction
Stress hormones can trigger uterine activity. Gentle yoga, breathing exercises, or even a favorite podcast can lower cortisol levels. A calm mind often translates to a calmer uterus. If you have concerns about how stress affects conditions like gestational diabetes, see resources on stress gestational diabetes for practical strategies.
RealWorld Story
Sarah, a 28yearold firsttime mom, noticed contractions at 32weeks. After switching to leftside sleep, cutting back on her daily 2hour commute, and practicing daily meditation, she bought an extra four days before her baby arrived. Those days meant a more mature lung profile and a smoother NICU stay.
Risks vs. Benefits of Delaying Labor
Benefits
- Full steroid course for lung maturity.
- Magnesium for brain protection.
- Time for transport to a higherlevel NICU.
- Potential for additional fetal growth.
Risks
- Medication side effects low blood pressure, heart rate changes.
- Possible infection if labor is suppressed too long.
- Maternal stress from prolonged hospitalization.
DecisionMaking Framework
Ask yourself and your provider:
- What is the babys gestational age?
- What is the underlying cause of contractions?
- Do the benefits of steroids and magnesium outweigh medication risks?
- Is a NICU transfer feasible within the delay window?
When to Seek Immediate Help
RedFlag Symptoms
- Contractions every 5minutes or less lasting >30seconds.
- Vaginal bleeding or gush of fluid.
- Severe, persistent abdominal pain.
- Rapid cervical change noted by a clinician.
Emergency Contact Template
Keep this script handy: Hi, Im pregnant at __ weeks and Im experiencing regular contractions that are ___ minutes apart. I think I may be in preterm labor. Have your OBGYNs number, the nearest labor&delivery unit, and a trusted family members contact ready.
Conclusion
In short, how long can preterm labor be delayed depends on many moving pieces gestational age, the cause of labor, and the specific medication used. Typically, doctors can pause contractions for 48hours to a week, buying critical time for steroids, magnesium, and transport to a NICU. Understanding the signs, staying proactive about lifestyle tweaks, and keeping a clear line of communication with your care team are the best ways to turn those precious hours into a healthier start for your baby.
If youre facing preterm labor, remember youre not alone. Reach out to your provider at the first sign of trouble, and dont hesitate to ask questions knowledge is one of the most powerful tools you have. What has your experience been? Share your story in the comments or ask any question you have. Were all in this together.
FAQs
What is the typical maximum time doctors can delay preterm labor?
Most tocolytic medications can pause contractions for about 48 hours, and when combined with magnesium sulfate the delay can extend up to 5–7 days.
Which medications are most commonly used to delay preterm labor?
Nifedipine, indomethacin, and magnesium sulfate are the first‑line tocolytics. Nifedipine is often used first, indomethacin before 32 weeks, and magnesium sulfate for neuroprotection and additional delay.
Why is a 48‑hour delay considered the gold standard?
That window allows a full course of corticosteroids to mature the baby’s lungs, which significantly reduces respiratory complications after birth.
Can lifestyle changes help prolong a pregnancy that is going into preterm labor?
While lifestyle measures (left‑side sleeping, hydration, reduced stress, and limited heavy activity) can’t stop true preterm labor, they may lessen uterine irritability and support overall maternal health.
When should a pregnant person call emergency services for possible preterm labor?
Call immediately if contractions occur every 5 minutes or less, are accompanied by vaginal bleeding, fluid leakage, severe pain, or rapid cervical change.