Hey there, future mom! If youve just been told your blood test shows low platelets and the doctor mentioned gestational thrombocytopenia, youre probably feeling a mix of relief (its not something scary) and confusion (what does this mean for my baby?). Lets cut through the medical jargon together and give you the clear, friendly rundown you deserve.
What Is Gestational Thrombocytopenia?
In plain English, gestational thrombocytopenia (often shortened to GT) is a mild, pregnancyrelated dip in platelet count. Platelets are the little blood cells that help clot blood when you scrape a kneeor when youre about to give birth. During pregnancy, its normal for the blood to get a bit diluted, and that can push platelet numbers down a little.
Most women with GT never notice any symptoms. The condition shows up on routine blood work, usually in the second or third trimester, and it typically resolves on its own after delivery. Think of it as a temporary traffic jam in your bloodstream that clears once the baby arrives.
Causes and Risk Factors
GT isnt caused by a disease so much as a combination of pregnancyspecific changes:
- Increased plasma volume: Your body holds more fluid to support the growing baby, which dilutes platelets.
- Hormonal shifts: Estrogen and progesterone subtly affect how platelets are produced and cleared.
- Mild splenic sequestration: The spleen may hold onto a few more platelets than usual.
These factors are why GT is considered a benign conditiontheres no underlying disease to treat, just a physiological adjustment.
Gestational Thrombocytopenia vs. ITP
Its easy to mix up GT with immune thrombocytopenic purpura (ITP), especially because both involve low platelets. The key differences are:
| Feature | Gestational Thrombocytopenia (GT) | Immune Thrombocytopenic Purpura (ITP) |
|---|---|---|
| Typical Platelet Count | 10015010/L (often 13015010/L) | Often <5010/L, can be <2010/L |
| Onset | 2nd3rd trimester | Any time, sometimes before pregnancy |
| History of low platelets | Rare | Common |
| Response to steroids | Usually none needed | Often improves with steroids |
When your platelet count falls below 5010/L, clinicians will usually investigate for ITP or other serious causes. , this threshold prompts a deeper workup rather than assuming GT.
Symptoms (or Lack Thereof)
Most women with GT dont experience any symptoms at all. If you do notice something, its usually mild and nonspecific:
- Occasional pinprick bruises
- Minor gum bleeding after flossing
- Rarely, tiny red spots (petechiae) on the skin
Redflag signs that merit immediate medical attention include heavy vaginal bleeding, sudden bruising without cause, severe headache, or visual changes. These could point to a more serious condition like preeclampsia or HELLP syndrome rather than GT.
Diagnosis and PlateletCount Interpretation
Diagnosing GT is essentially a process of elimination:
- Complete blood count (CBC): Your obstetrician will spot the low platelet number.
- Repeat testing: A second CBC a few weeks later confirms that the count is stable and not rapidly falling.
- Ruleout other causes: Blood pressure checks, urine protein tests, and a review of any medications youre taking.
Heres a quick guide to what the numbers usually mean:
- 15010/L: Normal range; no action needed.
- 10014910/L: Classic GT range; monitor every 46 weeks.
- 509910/L: Possible GT but warrants closer surveillance and a hematology consult.
- <5010/L: Alarm zone; investigate for ITP, preeclampsia, infection, or medication effects.
A visual timeline often helps expectant parents understand how platelets behave across pregnancy. Imagine a gentle slope that starts around 15010/L in the first trimester, eases down to roughly 12010/L by week30, and then rebounds to normal levels a few weeks after delivery.
Management and Treatment Options
The good news? GT rarely needs treatment. Your care plan will usually look like this:
When No Treatment Is Needed
If your platelet count stays above 10010/L and you have no bleeding, the standard approach is watchful waiting. Routine CBCs every month or so keep the situation on the radar, and you can continue your prenatal visits as usual.
When to Consider Intervention
Intervention is only considered if your count dips below the safety thresholds for delivery or anesthesia, or if you develop any bleeding complications. In those cases, the options include:
- Corticosteroids: Helpful for ITP, not typically for pure GT.
- Intravenous immunoglobulin (IVIG): Reserved for severe immunemediated thrombocytopenia.
- Platelet transfusion: Only in emergencies (e.g., active hemorrhage or before a cesarean section when counts are <5010/L).
Guidelines from the and the both stress that treatment should be individualized and that most GT cases are managed expectantly.
Pregnancy Course, Delivery Planning, and Neonatal Considerations
How does GT affect the third trimester and the actual birth?
ThirdTrimester Platelet Trends
Platelet counts often dip a bit more in the third trimester because plasma volume peaks. This is why many obstetricians order a CBC around week2832. For most women, the count stays comfortably above 8010010/L, which is considered safe for most obstetric interventions.
Epidural and Spinal Anesthesia
Neuraxial anesthesia (the epidural you might want for labor pain) is generally safe if platelets are 8010010/L. , counts lower than this raise a modest risk of spinal hematoma, so anesthesiologists may opt for a lowdose epidural or consider a general anesthetic if the count is too low.
Cesarean Section Decisions
GT alone is not an indication for a Csection. Your obstetric team will decide based on the usual obstetric indications (position of the baby, labor progress, etc.). If a surgical delivery is needed and platelets are borderline, they might give a platelet transfusion just to keep the surgical team comfortable.
Newborn Platelet Counts
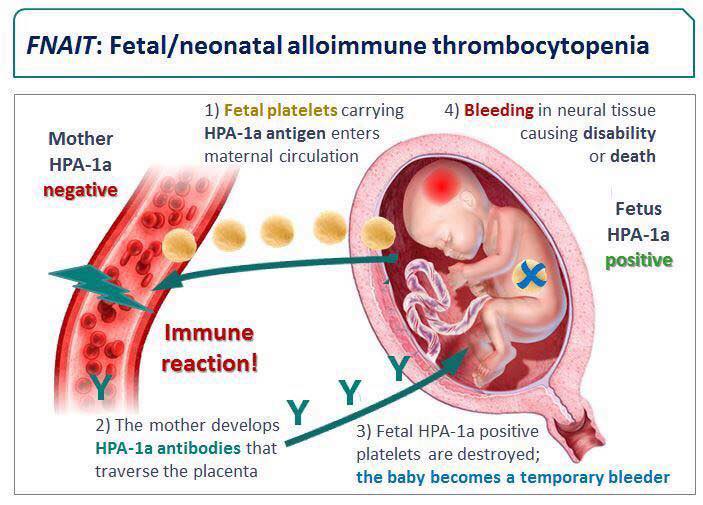
Babies born to mothers with GT typically have normal platelet counts. In the rare event that a newborns platelets are low, its usually a transient neonatal alloimmune thrombocytopenia and not directly linked to the mothers GT.
RealWorld Experiences (Adding Authority and Relatability)
Sarahs Story
Sarah, a 32yearold firsttime mom, recalls the moment she got her lab results: I was in the kitchen making tea when the nurse called. Your platelets are a bit low, but its probably gestational thrombocytopenia. My heart stopped for a secondwhat does that mean for my baby? After a quick chat with her OB, she learned that her count was 13810/L, perfectly safe. She kept a simple diary of her CBC results, and the numbers stayed steady until she delivered a healthy baby boy.
Clinician Insight
Dr. Maya Patel, a maternalfetal medicine specialist, says, What scares patients most is the unknown. By explaining the typical platelet trajectory and reassuring them that GT resolves after delivery, we reduce anxiety and avoid unnecessary interventions. She recommends a CBC at 28 weeks and a followup at 34 weeks for anyone with platelets below 12010/L.
Resources and How to Stay Informed
Trusted sources are essential for making confident decisions. Here are a few you can explore whenever you need a deeper dive:
Feel free to download a printable GT monitoring chart (just ask your provider for a copy) and keep it in your prenatal binder. Having a clear visual can make each appointment feel less like a mystery.
Conclusion
Gestational thrombocytopenia is a common, usually harmless dip in platelets that shows up in the second or third trimester. Knowing the typical platelet ranges, recognizing redflag symptoms, and following the evidencebased guidelines from ACOG, RCOG, and NICE equips you to stay relaxed and focused on the excitement of welcoming your baby. Most importantly, remember youre not aloneyour healthcare team, reputable resources, and other moms whove walked this path are all here to support you.
What questions do you still have about low platelets during pregnancy? Share your thoughts or personal experiences in the comments below, and lets keep the conversation going. If anything feels unclear, dont hesitate to ask your OBGYNtheyre the best source for personalized advice.
FAQs
What is gestational thrombocytopenia and how common is it?
Gestational thrombocytopenia (GT) is a mild, pregnancy‑related decrease in platelet count that usually occurs in the 2nd or 3rd trimester. It affects about 5‑10 % of pregnant women and typically resolves after delivery.
How can I tell if my low platelet count is GT or something more serious?
GT usually shows platelet numbers between 100‑150 × 10⁹/L, has no prior history of low platelets, and appears late in pregnancy. Counts below 50 × 10⁹/L, a sudden drop, or accompanying symptoms (heavy bleeding, severe headache) require further evaluation for conditions like ITP, preeclampsia, or HELLP.
Will gestational thrombocytopenia affect my delivery plan?
Most women with GT can have a normal vaginal delivery and safely receive an epidural if platelets are ≥ 80‑100 × 10⁹/L. GT alone is not an indication for a cesarean section; the decision is based on usual obstetric reasons.
Do I need any medication or special treatment for GT?
Generally no. GT is managed with observation and periodic CBC checks. Treatment (steroids, IVIG, platelet transfusion) is reserved for severe thrombocytopenia (< 50 × 10⁹/L) or bleeding complications, which are rare in pure GT.
Will my baby have low platelets because of my GT?
Newborns of mothers with GT almost always have normal platelet counts. If a baby does show low platelets, it is usually due to a different condition such as neonatal alloimmune thrombocytopenia, not the mother’s GT.