Imagine sitting in the doctors office, hearing the words your blood pressure is 150/95mmHg for the first time in your pregnancy. Your mind races is my baby safe? The quick answer is: yes, most women with gestational hypertension can have healthy babies when the right steps are taken. Below, Ill walk you through everything you need to know, from what the condition really means to the medicines, lifestyle tweaks, and delivery plans that keep you and your little one thriving.
What Is Gestational Hypertension
Simple definition
Gestational hypertension is high blood pressure that appears after 20weeks of pregnancy and usually disappears after delivery. Its different from chronic hypertension, which exists before pregnancy.
How common is it?
About 68% of pregnant people develop this condition, according to a recent . That means youre definitely not alone.
Why does it happen?
During pregnancy, your blood volume rises by up to 50%. Hormones also cause your blood vessels to relax. In some people, these changes raise the pressure on the arterial walls, leading to gestational hypertension.
Whos at risk?
- First pregnancy (nulliparity)
- Age>35years
- Prepregnancy obesity or excess weight gain
- Family history of hypertension or preeclampsia
- Multiplegestation (twins, triplets)
Quick tip: If any of these sound familiar, bring them up at your next prenatal visit. Knowing your risk helps the care team plan ahead.
Gestational Hypertension vs Preeclampsia
Key differences at a glance
| Feature | Gestational Hypertension | Preeclampsia |
|---|---|---|
| Blood pressure threshold | 140/90mmHg after 20weeks | 140/90mmHg + proteinuria or organ signs |
| Protein in urine | Usually absent | Present (300mg/24h) |
| Organ involvement | Rare | Kidneys, liver, brain, placenta |
| Progression risk | 20% develop preeclampsia | Already established |
Why the distinction matters
Both conditions need careful monitoring, but preeclampsia often calls for earlier delivery or stronger medication. Knowing which side of the fence youre on guides the treatment plan.
Symptoms & Warning Signs
Typical symptoms you might notice
- Persistent headache (not just mom brain)
- Blurred or flashing vision
- Sudden swelling (especially face or hands)
- Rapid weight gain (>2kg in a week)
- Upper abdominal pain
Silent cases are common
Up to half of the people with gestational hypertension feel perfectly fine. Thats why routine prenatal bloodpressure checks are crucial they catch the silent cases before complications arise.
Redflag signs that need immediate care
- BP160/110mmHg
- Severe headache or visual changes
- Persistent vomiting or abdominal pain
- Reduced fetal movements
If any of these happen, call your provider right away or head to the emergency department. Quick action can protect both you and the baby.
Treatment Guidelines
What professional bodies recommend
The 2024 American College of Obstetricians and Gynecologists (ACOG) guideline and the 2023 NICE guideline both stress three pillars: regular monitoring, appropriate medication when BP150/100mmHg, and individualized delivery timing. offers a concise snapshot.
Monitoring schedule
- Home BP checks: at least twice daily (morning & evening)
- Clinic visits: every 12weeks if BP is stable, weekly or more if it rises
- Fetal surveillance: nonstress test & growth ultrasounds every 24weeks
Hospitalization criteria
Doctors may admit you if you have:
- Severe hypertension (160/110mmHg) despite meds
- Signs of organ dysfunction (elevated liver enzymes, low platelets)
- Uncontrolled pain or persistent vomiting
Bedrest does it help?
Evidence is mixed. Light activity (short walks) is usually better than strict bedrest, which can increase clot risk. Some hospitals still prescribe modified rest (limited standing, frequent sitting) for severe cases.
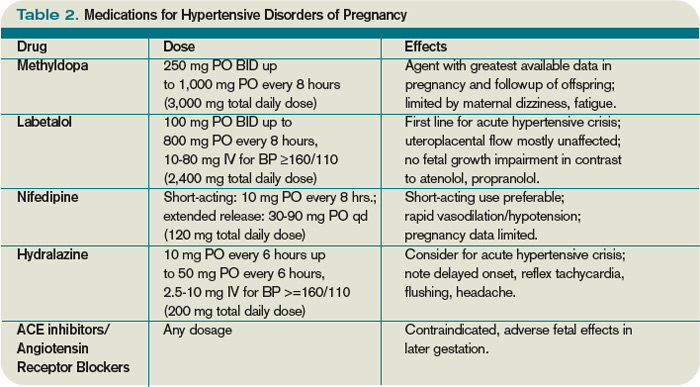
FirstLine Medications
Drug classes considered safe in pregnancy
- Methyldopa longstanding, low sideeffect profile
- Labetalol combined and blocker, fast onset
- Shortacting nifedipine calciumchannel blocker, useful for quick BP control
How doctors choose which one
They look at your BP level, any existing conditions (like asthma or diabetes), and how you tolerate side effects. For example, a patient with asthma may avoid blockers and opt for nifedipine.
Typical dosing (always follow your providers order)
| Medication | Starting Dose | Usual Max Dose | Common Sideeffects |
|---|---|---|---|
| Methyldopa | 250mg PO BID | 1g PO QID | Drowsiness, dry mouth |
| Labetalol | 100mg PO BID | 2.4g PO/IV per day | Fatigue, dizziness |
| Nifedipine (shortacting) | 10mg PO q6h PRN | 3040mg PO q6h | Flushing, headache |
When medication isnt needed yet
If your BP stays below 150/100mmHg and you have no organ concerns, many clinicians recommend close monitoring without drugs. This watchful waiting approach protects you from unnecessary medication exposure.
Lifestyle Strategies
Diet tweaks that help
Salt isnt the enemy, but excess sodium can exacerbate hypertension. Aim for <2,300mg of sodium daily thats about one teaspoon of salt. Load up on potassiumrich foods (bananas, sweet potatoes, beans) which naturally counterbalance sodium.
Safe exercise ideas
Unless your provider says otherwise, 150 minutes of moderate activity each week is fine. Think brisk walking, prenatal yoga, or swimming. The key is consistency, not intensity.
Stressreduction tools
Stress hormones can raise blood pressure, so try breathing exercises, guided meditation apps, or simply a nightly unplug routine. Even a 5minute mindful pause can lower systolic numbers by a few points.
Home bloodpressure monitoring
Pick a validated cuff (look for validated for pregnancy on the packaging). Record readings in a notebook or app, noting the time, position (sitting upright), and any symptoms. When you see a trend upward, call your obstetrician.
Complications & Delivery Planning
Possible complications if untreated
- Placental abruption (premature detachment)
- Preterm birth
- Intrauterine growth restriction (IUGR)
- Future cardiovascular disease for mother
Delivery options and odds of a vaginal birth
Most people with wellcontrolled gestational hypertension can have a vaginal delivery. According to , the chance of a normal delivery is roughly 7080% when BP is managed.
However, if severe hypertension or preeclampsia develops, early induction (often at 3738weeks) or a Csection may be recommended for safety.
Postpartum followup
Blood pressure usually normalizes within 612weeks after delivery, but a followup visit is essential. Women who had gestational hypertension are at higher risk for chronic hypertension later in life, so your doctor may suggest lifestyle monitoring or lowdose medication longterm.
Common Questions Answered
Can I stay on my prepregnancy bloodpressure pills?
Most chronic hypertension meds (like ACE inhibitors) are unsafe in pregnancy. Your provider will likely switch you to methyldopa, labetalol, or nifedipine, which have solid safety data.
How long will I need medication?
Usually until delivery, then a short taper if BP stays normal. Some women continue lowdose therapy postpartum if their numbers stay high.
Is it safe to breastfeed while on these drugs?
Yes. Methyldopa, labetalol, and shortacting nifedipine are considered compatible with breastfeeding; only trace amounts pass into milk.
Will high blood pressure affect my babys health?
When wellcontrolled, the risk of growth restriction or preterm birth is low. Regular fetal growth ultrasounds keep you and the care team informed.
Can lifestyle alone control my blood pressure?
In many mild cases, diet, gentle exercise, and stress control can keep BP in the target range. However, its wise to have a medication plan ready if numbers creep upward.
Putting It All Together
Gestational hypertension can feel like an unexpected hurdle, but its one you can navigate with knowledge, support, and a solid treatment plan. Heres a quick recap:
- Know the signs. Regular BP checks and awareness of symptoms are your first line of defense.
- Follow evidencebased guidelines. ACOG and NICE provide clear thresholds for when medication is needed.
- Choose safe meds. Methyldopa, labetalol, and shortacting nifedipine are the goto options.
- Embrace lifestyle tweaks. Lowsalt meals, gentle movement, and stressrelief practices complement any prescription.
- Plan delivery wisely. With proper control, most people have a vaginal birth; severe cases may need earlier induction or Csection.
- Stay vigilant after birth. Followup visits help ensure your blood pressure stays normal and flag any longterm hearthealth concerns.
Remember, youre not alone on this journey. Your healthcare team, supportive friends, and trusted resources are all here to help you cross the finish line safely.
Whats been your experience with bloodpressure monitoring during pregnancy? Share your story in the comments, ask any lingering questions, or just say hi. Im here to listen and help you every step of the way.
FAQs
What blood‑pressure level triggers medication for gestational hypertension?
Doctors usually start medication when readings reach 150/100 mm Hg or higher, or if the pressure spikes quickly.
Are methyldopa, labetalol, and nifedipine safe for the baby?
Yes, these three drugs have extensive safety data and are considered compatible with pregnancy and breastfeeding.
Can I control gestational hypertension with diet and exercise alone?
In mild cases, low‑salt meals, regular gentle activity, and stress‑relief can keep numbers in range, but medication may still be needed if pressure rises.
How often should I monitor my blood pressure at home?
Check twice daily (morning and evening) using a validated cuff, recording the time, position, and any symptoms.
When is delivery recommended for someone with gestational hypertension?
If blood pressure stays controlled, delivery can follow the usual schedule; severe hypertension or progression to preeclampsia often leads to induction around 37‑38 weeks.