Quick Answer
If youve just heard the phrase FIGO grade2 treatment, the short answer is: most women start with surgerytotal hysterectomy with removal of both ovariesand then consider radiation only if certain risk factors are present. In many cases, the surgery alone is enough to give a very good chance of cure.
Why Grade Matters
What does FIGO grade2 mean?
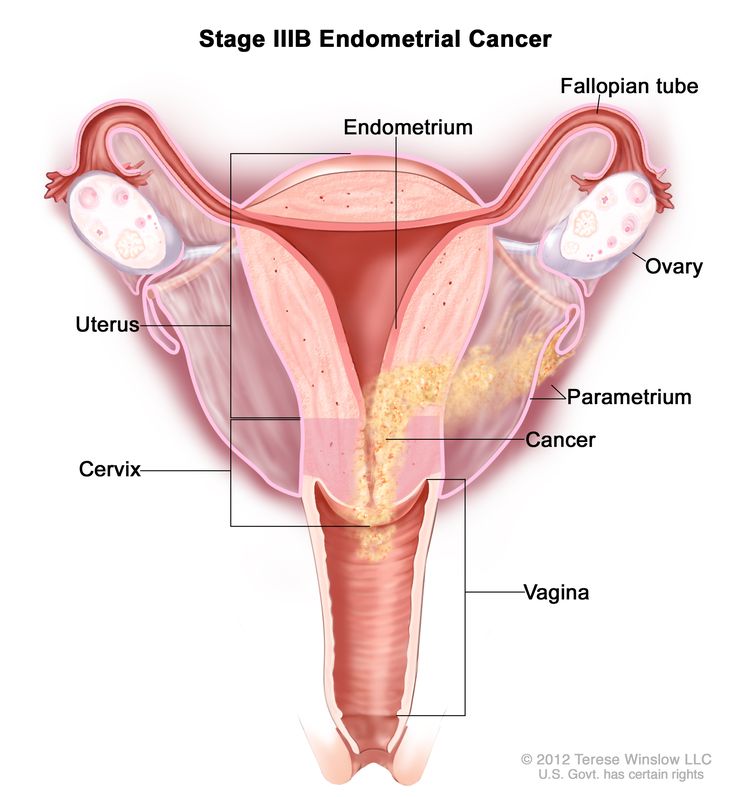
FIGO (International Federation of Gynecology and Obstetrics) grades endometrial tumors based on how much of the tissue looks like normal glands. Grade2 sits in the middle: roughly 650% of the tumor shows solid, nonglandular growth. Its more aggressive than grade1 but not as aggressive as grade3.
How does grade affect prognosis?
Studies consistently show that women with grade2 disease, especially when caught at an early stage (stageIII), enjoy a fiveyear survival rate above 85%. The risk of the cancer coming back is higher than with grade1 but still far lower than the 50plus percent seen with grade3. In plain language, grade2 is the middle child it needs attention, but the outlook is usually usually very positive when treated correctly. For patients considering longterm outcomes after removing reproductive organs, reading about survival without prostate can provide perspective on recovery and quality of life after major cancer surgery.
Realworld example
Take Maya, a 58yearold who was diagnosed after a routine pelvic exam. Her tumor was classified as FIGO grade2, stageIB. She underwent a total hysterectomy with bilateral salpingooophorectomy and, because no highrisk features were found, she did not receive radiation. Two years later shes cancerfree and back to gardening on weekends. Stories like Mayas remind us that grade2 often means treatable and survivable.
Surgery First
What surgery is recommended?
The cornerstone of FIGO grade2 endometrial cancer treatment is a total hysterectomy (removal of the uterus) plus bilateral salpingooophorectomy (removal of both ovaries and fallopian tubes). Many surgeons also remove pelvic and sometimes paraaortic lymph nodes to see if the cancer has spread.
Do I need lymphnode removal?
Not every patient. Current guidelines suggest a riskadjusted approach: if the tumor is deeply invasive or shows lymphvascular space involvement, nodes are usually taken. If the tumor is shallow and lowrisk, the surgeon may skip it to reduce surgical morbidity.
Preparing for surgery a checklist
| Step | Why it matters |
|---|---|
| Preop blood work | Checks anemia, kidney function, clotting |
| Imaging (CT/MRI) | Looks for spread beyond the uterus |
| Fertility discussion | Important if youre considering future pregnancy |
| Ask about pain control plan | Helps you recover faster |
Radiation Choices
When is radiation needed?
Radiation isnt automatically added for every FIGO grade2 case. It becomes a partner when you have any of the following:
- Deep myometrial invasion (beyond half the uterine wall)
- Lymphvascular space involvement
- Positive or close surgical margins
- Unfavorable histology (e.g., serous features)
Internal brachytherapy vs. external beam
Vaginal brachytherapy delivers radiation directly to the top of the vagina, sparing nearby organs. Its the goto for many earlystage, grade2 women who need extra insurance against local recurrence. Externalbeam radiation therapy (EBRT) covers a larger areapelvis and sometimes abdomenand is reserved for higherrisk scenarios.
What the research says
A large analysis of over 4,000 patients showed that adding vaginal brachytherapy to surgery reduced vaginal recurrences without a survival benefit for lowrisk stage1AG2 disease. In other words, if youre lowrisk, you might skip radiation altogether and still do great.
Decisionmaking flowchart (simplified)
Step1: Surgery completed.
Step2: Does pathology show any highrisk features?
- No Observation (no radiation).
- Yes Discuss brachytherapy (if risk limited to vagina) or EBRT (if deeper spread).
Chemo & Targeted
Is chemotherapy necessary for grade2?
Usually not for earlystage (III) disease if the surgery removed everything cleanly. Chemotherapy becomes part of the plan for stageIIIII disease, especially when nodes are positive or the tumor shows aggressive behavior.
Typical regimen
The standard combo is carboplatin plus paclitaxel, given every three weeks for 36 cycles. This partnership attacks cancer cells that might be hiding after surgery.
New horizons: immunotherapy and HER2
Researchers are testing pembrolizumab (an immune checkpoint inhibitor) and trastuzumab (an HER2targeted drug) for highgrade endometrioid cancers that overexpress HER2. The trials are promising, but theyre still experimental for most grade2 patients.
Quick tip
If your doctor mentions chemo, ask about the expected sideeffects, duration, and whether a clinical trial might be a better match for your situation.
FollowUp Care
Surveillance schedule
After you finish treatment, the usual followup looks like this:
- Every 34months for the first 2years
- Every 6months for years35
- Annually thereafter
Each visit typically includes a pelvic exam, a look at any vaginal cuff cytology, and imaging only if something feels off.
Redflag signs
Call your doctor right away if you notice:
- Pain or pressure in the pelvis
- Unusual bleeding or discharge
- Sudden weight loss or fatigue
Emotional checkpoint
Its normal to feel a little jittery during those first months. Many patients find comfort in joining support groups (online or inperson) where stories like Mayas become a source of hope and practical tips.
Balancing Benefits & Risks
Benefits of surgeryfirst
Removing the primary tumor gives the best chance for cureusually over an 85% fiveyear survival for earlystage grade2 disease. It also provides the most accurate pathology, which guides any further treatment.
Potential downsides
Major surgery carries risks: bleeding, infection, and a permanent menopause if the ovaries are removed. Radiation can cause bowel or bladder irritation, and chemotherapy brings nausea, fatigue, and hair loss. The key is to weigh these sideeffects against the added protection they might give.
Questions to ask your oncologist
- Do I have any highrisk features that would make radiation worthwhile?
- What are the chances of recurrence with surgery alone?
- How will menopause affect my longterm health, and can hormone therapy be considered?
- Are there clinical trials suitable for me?
Patientcentered decision aid
Put pen to paper (or phone notes) and list your prioritieslongevity, quality of life, fertility, recovery time. Compare each treatment option against those priorities. This simple exercise often clears the fog and empowers you to make a confident choice.
Conclusion
FIGO grade2 endometrial cancer sits in that middle ground where treatment is both effective and nuanced. Most women achieve excellent outcomes with a hysterectomy and bilateral oophorectomy; radiation is added only when particular risk factors tip the scales. Chemotherapy and newer targeted therapies step in for more advanced stages. By staying informed, asking the right questions, and partnering with a trusted gynecologic oncologist, you can navigate the journey with confidence and hope. If youre ready to dive deeper, consider downloading a free treatmentdecision checklist or reaching out to a nurse navigator for personalized guidance.
FAQs
What is the standard initial treatment for FIGO grade 2 endometrial cancer?
The primary treatment is a total hysterectomy with bilateral salpingo-oophorectomy, often including pelvic lymph node assessment depending on risk factors.
When is radiation therapy recommended after surgery for FIGO grade 2?
Radiation is considered if there is deep myometrial invasion, lymphovascular space involvement, close or positive surgical margins, or unfavorable histology features such as serous differentiation.
Is chemotherapy commonly used for FIGO grade 2 endometrial cancer?
Chemotherapy is generally reserved for more advanced stages (stage III and above) or if nodes are positive; it is not typical for early-stage grade 2 disease after complete surgical removal.
What are the follow-up recommendations after treatment for FIGO grade 2?
Follow-up usually includes pelvic exams every 3–4 months for the first 2 years, every 6 months for years 3–5, then annually, with imaging as needed based on symptoms.
How does FIGO grade 2 affect prognosis compared to other grades?
Grade 2 tumors are intermediate in aggressiveness, with about an 85% five-year survival rate for early-stage disease—higher risk than grade 1 but better outlook than grade 3.