If youve ever typed worst type of lymphoma into a search box, youre probably looking for a quick, clear answer: the most aggressive lymphomas grow fast, act like a sprint rather than a marathon, and need immediate treatment. Below youll find a friendly guide that tells you which subtypes are the toughest, how doctors spot them, and what the newest therapies mean for survival. Lets dive in together no jargon, just the facts you need.
Quick Primer
What Makes a Lymphoma Aggressive?
In the world of lymphomas, aggressive (or highgrade) refers to cancers that double in size within weeks, cause symptoms quickly, and require prompt therapy. According to , aggressive lymphomas are usually nonHodgkin (NHL) varieties that need intensive chemoimmunotherapy right away.
Aggressive vs. Indolent: The Core Differences
- Growth rate: Aggressive = rapid; Indolent = slowgrowing.
- Symptoms: Aggressive often brings fever, night sweats, weight loss (the dreaded Bsymptoms) in weeks; indolent may be silent for years.
- Treatment urgency: Aggressive needs immediate action; indolent can sometimes be watched.
SidebySide Comparison
| Feature | Aggressive (HighGrade) NHL | Indolent (LowGrade) NHL |
|---|---|---|
| Typical growth | Weeks to months | Months to years |
| Common subtypes | DLBCL, Burkitt, Mantlecell | Follicular, Smalllymphocytic |
| 5year survival (average) | 60% | 80% |
| Firstline therapy | Chemoimmunotherapy (RCHOP, EPOCHR) | Watchful waiting or mild chemo |
The Worst Lymphoma Types
Burkitt Lymphoma The Speedster
Burkitt is often called the fastestgrowing lymphoma on the planet. It can double in size within 2448 hours! Though rare, it mainly hits children and young adults. If caught early, intensive shortcourse chemo can push 5year overall survival (OS) up to 80%.
Key Facts
- Incidence: Less than 1% of all lymphomas.
- Typical age: 530years.
- Genetics: MYC translocation (t[8;14]).
- Treatment: Short, highdose chemo (e.g., CODOXM/IVAC).
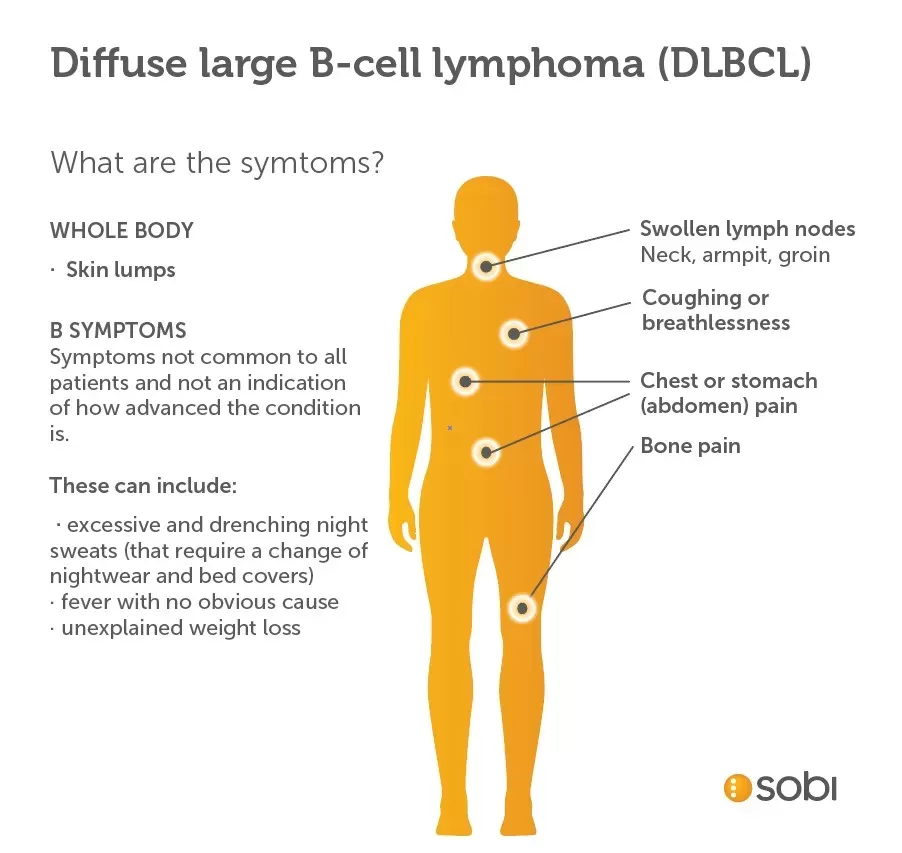
Diffuse Large BCell Lymphoma (DLBCL) The Most Common Aggressive NHL
DLBCL accounts for roughly 30% of all adult lymphomas, making it the most common worsttype in the United States. Its rapid progression and diversity of presentations earn it a spot on most worst type of lymphoma lists.
Why DLBCL Gets the Spotlight
- Prevalence: 12cases per 100,000 people each year.
- Standard regimen: RCHOP (rituximab+cyclophosphamide+doxorubicin+vincristine+prednisone).
- Response rates: 6070% achieve complete remission.
- Median OS: Around 57years with modern therapy.
MantleCell Lymphoma The RelapseProne Threat
Often showing up in people over 60, mantlecell is a worst contender because it likes to come back even after a good response. Its hallmark is the t(11;14) translocation, which drives cyclin D1 overexpression.
Prognosis Snapshot
- Median OS: 35years without newer agents.
- Emerging therapy: BTK inhibitors (ibrutinib, acalabrutinib) have extended survival for many.
- Typical presentation: Enlarged lymph nodes, sometimes a bulky abdomen.
Primary Mediastinal BCell Lymphoma The Young Adult Challenge
Although it shares pathology with DLBCL, this subtype often hits people in their 20s30s and forms a large mass in the chest, causing breathing trouble and severe Bsymptoms.
What Works Best?
Doseadjusted EPOCHR (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin+rituximab) shows cure rates above 80% in recent trials.
Rare Aggressive NonHodgkin Lymphomas
Lymphoblastic Lymphoma (Tcell & Bcell)
Think of it as a hybrid of lymphoma and acute lymphoblastic leukemia. It spreads quickly, and without stemcell transplant the 5year survival can dip below 50%.
NK/TCell Lymphoma (Nasal Type)
Most common in East Asia, this lymphoma loves the nasal passages and can cause destructive midline facial lesions. Combined radiation and chemo gives the best chance, yet the 5year OS remains under 40%.
Plasmablastic Lymphoma
Strongly linked to HIV infection, its notoriously aggressive and often resistant to standard chemo. Newer agents like bortezomib are being studied to improve outcomes.
Quick Reference Table
| Rare Aggressive Subtype | Typical Age | Key Genetic Marker | Standard FirstLine | 5Year OS |
|---|---|---|---|---|
| Lymphoblastic | Teens30s | NOTCH1, Tcell receptor | HyperCVAD | 45% |
| NK/TCell (nasal) | 2050yrs | EBVpositive | Radiation + DeVIC | 35% |
| Plasmablastic | 3060yrs (HIV+) | MYC rearrangement | EPOCHlike | 30% |
Spotting the Worst Type Signs, Diagnosis & Tests
RedFlag Symptoms You Shouldn\'t Ignore
When lymph nodes swell rapidly, you start sweating at night, lose weight without trying, and feel a fever that wont quit those are the classic Bsymptoms signaling an aggressive lymphoma. Trust your gut; early medical attention can save precious time.
How Doctors Confirm the Diagnosis
First, a PETCT scan maps the diseases spread. Then an excisional biopsy (a whole node, not just a needle) lets pathologists check cell morphology and run immunophenotyping. Molecular tests (FISH, PCR) hunt for specific translocations like MYC, BCL2, or t(11;14). The result? A precise lymphoma types chart that guides treatment.
Treatment Landscape Balancing Benefits & Risks
Standard ChemoImmunotherapy (RCHOP)
RCHOP remains the backbone for DLBCL and many other aggressive lymphomas. It works well, but its not without side effects think shortterm hair loss, nausea, and, for older patients, a higher risk of heart strain from doxorubicin.
When DoseAdjusted EPOCHR Is Preferred
For primary mediastinal Bcell lymphoma, the continuous infusion schedule of EPOCHR hits cancer cells more evenly and reduces the chance of a bulky chest mass returning.
Targeted Therapies & SmallMolecule Inhibitors
Mantlecell patients now have BTK inhibitors like ibrutinib, which block a key survival pathway in the cancer cells. In 2023, the FDA approved zanubrutinib for relapsed mantlecell, offering a new lifeline for many.
CART Cell Therapy & Bispecific Antibodies
For those whose disease relapses after chemo, CART (e.g., axicabtagene ciloleucel) rewires a patients own Tcells to hunt down lymphoma. Its a gamechanger, but access can be limited by cost and the need for a specialized center.
Prognosis & Survival What the Numbers Really Mean
Aggressive Lymphoma Survival Rates Overview
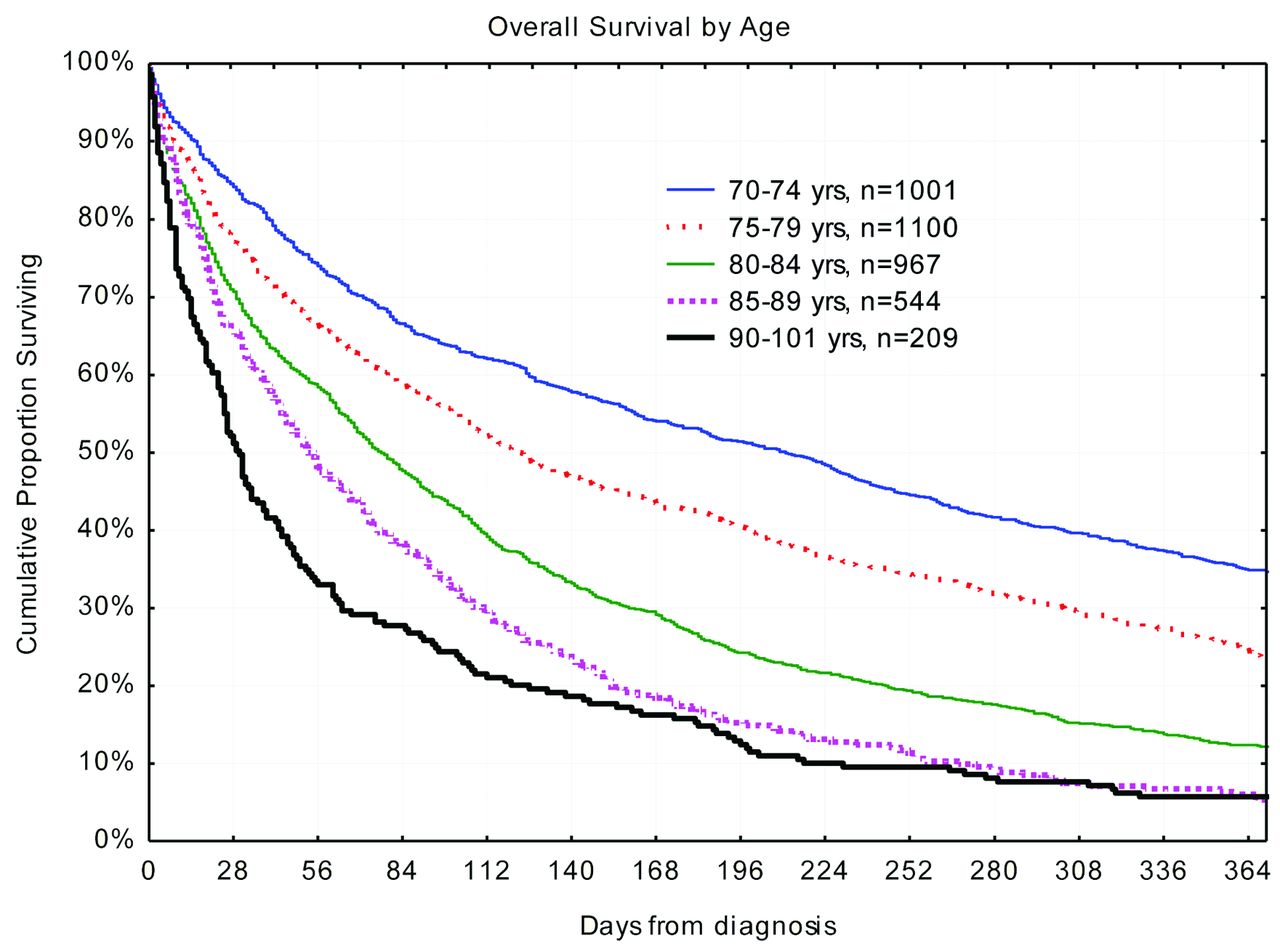
Overall, aggressive lymphomas have a 5year overall survival of roughly 60% when treated promptly. However, survival swings dramatically by subtype: Burkitt (80% with early therapy), DLBCL (70% with RCHOP), mantlecell (45% without BTK inhibitors, >60% with them).
Factors That Shift Outcomes
- Age: Patients over 70 often have lower tolerance for intensive chemo.
- Stage at diagnosis: Earlystage disease (III) can be curable; advanced (IIIIV) needs more aggressive regimens.
- Genetics: Doublehit lymphomas (MYC + BCL2/BCL6) have poorer prognosis.
- Performance status: How well a patient can carry out daily activities influences treatment choice.
Interactive Survival Calculator (Idea)
Imagine a simple widget where you enter age, stage, and subtype, and it spits out a personalized 5year survival estimate. While were not embedding one here, many cancer center websites already offer such tools.
RealWorld Experience Patient Stories & Case Studies
Case Study 1 19YearOld with Burkitt Lymphoma
Emily (name changed) noticed a painless lump in her neck that grew within a week. A biopsy confirmed Burkitt. She went straight into an intensive CODOXM regimen and, after six months, was declared in complete remission. Her story shows how rapid diagnosis + aggressive therapy can turn a frightening diagnosis into a hopeful outcome.
Case Study 2 62YearOld with DLBCL
John had a history of hypertension. He presented with night sweats and a swollen abdomen. PETCT revealed stage III disease. He received six cycles of RCHOP, but due to heart concerns, his oncologist adjusted the doxorubicin dose. John achieved remission and now enjoys gardening, proving that personalized dosing can keep both cancer and comorbidities in check.
Practical Takeaways
- Early recognition of Bsymptoms saves lives.
- Tailoring chemo intensity to age and heart health matters.
- Access to clinical trials can provide cuttingedge options.
Conclusion
The worst type of lymphoma isnt a single diseaseits a collection of fastgrowing, highgrade cancers like Burkitt, DLBCL, mantlecell, and several rare subtypes that demand swift, focused treatment. Knowing the warning signs, understanding how doctors diagnose these cancers, and being aware of the latest therapeutic options empower you to make informed decisions. If you or a loved one face an aggressive lymphoma, start a conversation with your oncology team, consider a second opinion, and lean on trusted resources such as the . Youre not alonesupport groups, research advances, and compassionate clinicians are all part of the journey toward better outcomes. For readers also managing prostate cancer questions, resources on prostate cancer outlook may help put prognosis and treatment decisions in context.
FAQs
What is considered the worst type of lymphoma?
The worst types of lymphoma are aggressive, fast-growing non-Hodgkin lymphomas such as Burkitt lymphoma, diffuse large B-cell lymphoma (DLBCL), and mantle cell lymphoma, which require immediate and intensive treatment.
Why are Burkitt lymphoma and DLBCL called aggressive lymphomas?
They are called aggressive because they grow rapidly, often doubling in size within days or weeks, causing symptoms quickly and needing prompt chemotherapy or chemoimmunotherapy to improve outcomes.
What is the typical survival rate for aggressive lymphomas?
Survival rates vary by subtype but generally, aggressive lymphomas have a 5-year overall survival rate around 60-70% with timely treatment; Burkitt lymphoma can reach up to 80% survival with early therapy.
How are the worst types of lymphoma diagnosed?
Diagnosis involves PET/CT scans to assess spread, excisional lymph node biopsy for morphology, immunophenotyping, and molecular tests to identify genetic markers like MYC or t(11;14) translocations guiding treatment decisions.
What are emerging treatments for aggressive lymphomas?
Besides standard chemoimmunotherapy, targeted therapies such as BTK inhibitors for mantle cell lymphoma and CART cell therapy for relapsed cases offer new hope, with ongoing research improving survival rates.