Imagine feeling a sudden, tearing pain in your chest right after a bout of vomiting, or noticing a weird crackling under your skin after an endoscopy. Those are the kind of warning signs that shouldn't be ignoredbecause a hole in the esophagus can become life-threatening in minutes. The good news? If you act fast, modern esophageal perforation treatment can dramatically lower the risk of death and get you back to normal eating much sooner than you'd think. For patients managing digestive health challenges, understanding symptoms and treatment options can be as crucial as knowing about ulcerative colitis supplements which support overall gut health.
Understanding the Emergency
What exactly is an esophageal perforation?
An esophageal perforation is a full-thickness tear in the wall of the esophagus, the tube that carries food from your mouth to your stomach. It's often called a ruptured esophagus, and it allows food, stomach acid, and bacteria to spill into the surrounding chest or neck spaces.
Why does it happen?
The causes are surprisingly varied. The most common culprits are:
- Instrument-related injuries during endoscopy or surgery
- Forceful vomiting (the classic Boerhaave syndrome)
- Blunt or penetrating chest trauma
- Swallowing sharp objects or caustic chemicals
What kinds of tears are there?
Doctors classify tears by location and depth. The three main esophageal tear types are:
| Location | Typical Symptoms | Typical Time to Diagnosis |
|---|---|---|
| Cervical (neck) | Neck pain, subcutaneous emphysema | 6 hours |
| Thoracic (chest) | Severe chest pain, shortness of breath | 612 hours |
| Abdominal (upper stomach) | Upper abdominal pain, fever | >12 hours |
Diagnosing the Perforation
What symptoms should raise alarm?
When a tear occurs, the body shouts out loud. Look for sudden, intense chest or neck pain, vomiting that won't stop, fever, difficulty swallowing, or a feeling of air bubbling under the skin (you can actually hear a crackling sound when you press on it). These esophageal perforation symptoms are red flags that demand immediate medical attention.
Which tests confirm the diagnosis?
Doctors usually start with a contrast esophagogramswallowing a dye that shows up on X-rayto pinpoint the leak. If the picture is hazy, a CT scan with oral contrast is the gold standard; it reveals not only the tear but also any fluid collections or mediastinal air. In some hospitals, a bedside endoscopy can directly visualize the rupture, but it's only done when the patient is stable enough.
When should you call emergency services?
If the pain starts after a bout of vomiting or a recent endoscopic procedure and you notice any of the symptoms above, dial 911 right away. Even if you're not sure, it's better to be safeearly treatment slashes the mortality rate from upwards of 40% down to under 10%.
Immediate Stabilization Steps
How does the ABC approach apply?
First things firstairway, breathing, circulation. The medical team will make sure you can breathe without obstruction, give you oxygen, and start IV fluids to keep blood pressure steady. You'll be told to stay NPO (nothing by mouth) to prevent more food from leaking into the chest.
Which meds are started right away?
Broad-spectrum IV antibiotics are a musttypically a combination that covers gram-positive, gram-negative, and anaerobic bacteria. Antisecretory agents (like proton pump inhibitors) are added to suppress stomach acid, reducing further damage.
What about pain control?
Managing pain is essential, both for comfort and to prevent shallow breathing that might lead to pneumonia. Doctors often use a balanced regimen of opioids (for severe pain) and nonopioid analgesics, monitored closely in an ICU setting.
Real-world example
John, a 45-year-old avid hiker, suddenly felt his chest split open after a prolonged bout of vomiting on a mountain trail. He was airlifted to a trauma center, where a chest tube drained the leaking fluid and a CT scan confirmed a thoracic tear. Within a few hours, he was on IV antibiotics and a nasogastric tubelaying the groundwork for definitive repair.
Definitive Treatment Options
When can you treat without surgery?
If the leak is tiny (<2cm), well-contained, and the patient is stable, doctors may opt for conservative management. This means continued antibiotics, close monitoring, and drainage of any fluid collections. Success rates for this approach hover around 70% when criteria are strictly met.
What does endoscopic stenting involve?
In many centers, an endoscopist will place a self-expanding metal or plastic stent across the tear. The stent acts like a bridge, sealing the hole while the tissue heals underneath. Studies show a high success rate, though complications such as stent migration can occur.
Which surgical routes are available?
When the tear is large, delayed, or the surrounding tissue is damaged, surgery becomes necessary. The main options are:
| Technique | When Used | Invasiveness | Typical Recovery |
|---|---|---|---|
| Primary thoracoscopic repair | Early (<24h), viable tissue | Minimally invasive | 23 weeks |
| Open esophagectomy with reconstruction | Extensive damage, >48h delay | Open/hybrid | 612 weeks |
| Hybrid (surgery+endoscopy) | Large tear, borderline tissue quality | Medium | 46 weeks |
How do doctors decide?
Imagine a flowchart in your mind: first ask, Is the patient stable? If yes, look at Size of leak. Small and contained? Go conservative. Bigger than 2cm or deteriorating? Consider stenting. If the leak is huge, the tissue looks bruised, or more than a day has passed, head to the OR. This decision tree helps keep the esophagus tear survival rate above 90% in experienced centers.
Recovery Timeline & Care
What's the typical recovery time?
After successful repair, most patients stay in the hospital for 510 days for IV antibiotics and monitoring. The esophageal perforation recovery time varies:
- Conservative treatment: 23 weeks before oral intake.
- Stent placement: 48 weeks before stent removal and gradual diet progression.
- Surgical repair: 36 weeks before soft foods, with full diet by 68 weeks.
How is nutrition managed?
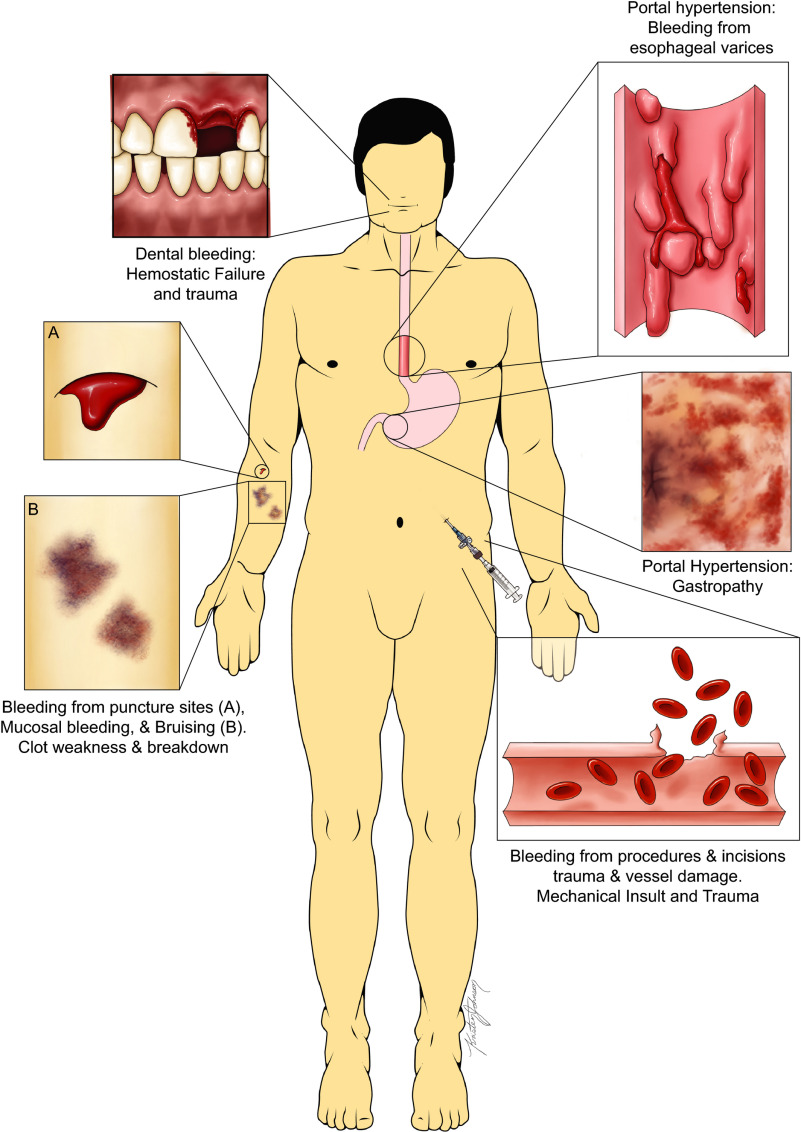
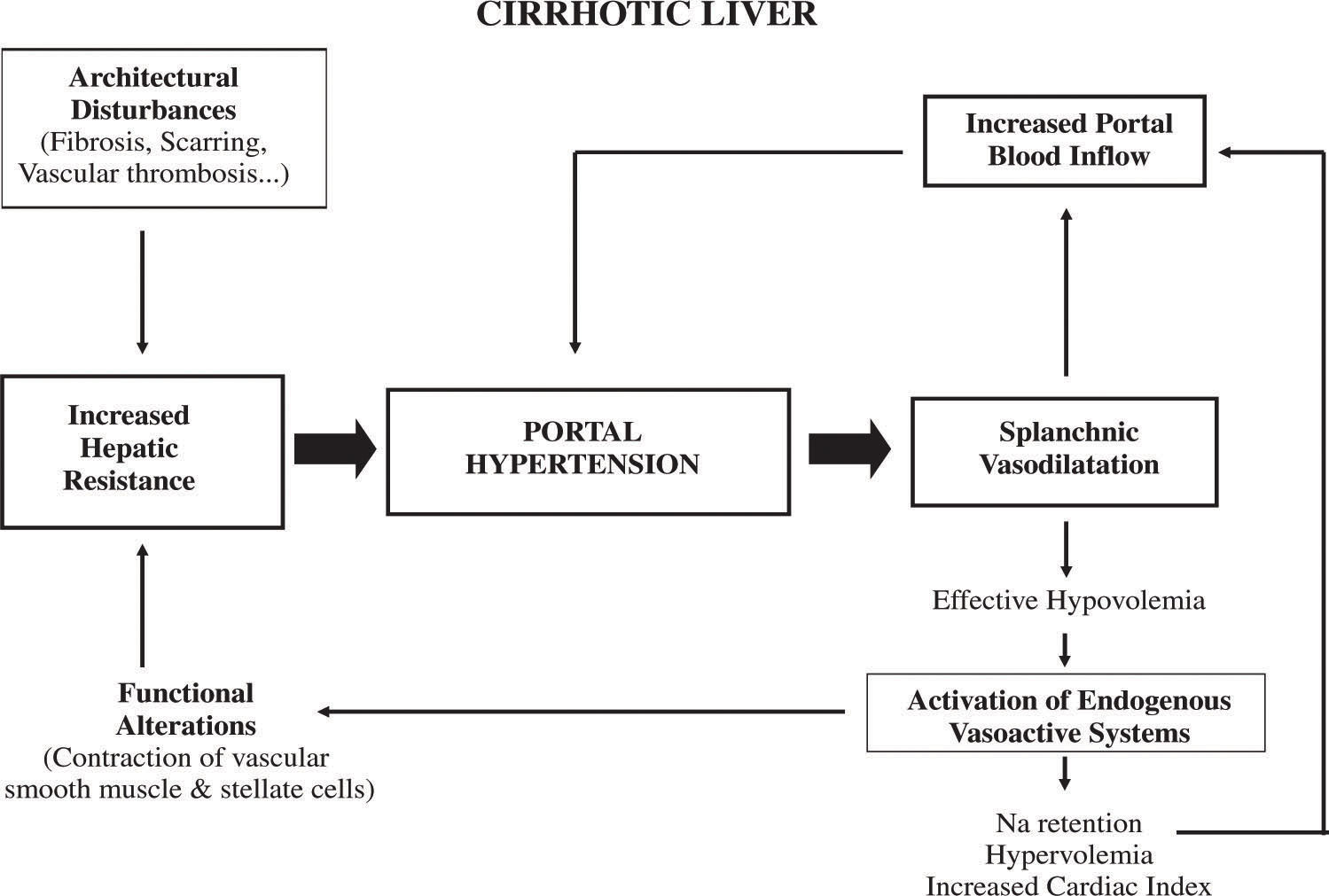
While the esophagus heals, nutrition is delivered intravenously or through a feeding tube placed past the tear (often a nasojejunal tube). A dietitian will tailor caloric needs, ensuring you don't waste precious energy on fighting malnutrition. Patients who have experience with digestive system conditions might also benefit from insights on Portal hypertension symptoms to monitor for related vascular complications.
What complications should you watch for?
Even after the hole is sealed, a few hurdles can appear:
- Stricture formation a narrowing that may need dilatation.
- Recurrent leak rare but possible if tissue didn't heal fully.
- Mediastinitis infection of the chest cavity, which is why the early antibiotics course is crucial.
Practical aftercare checklist
Here's a friendly reminder you can print out:
- Attend the follow-up endoscopy at 46 weeks.
- Avoid heavy lifting, hot liquids, and very spicy foods for at least 2 months.
- Stay on a proton pump inhibitor for 812 weeks to protect the repaired esophagus.
- Quit smoking it slows healing and raises the risk of strictures.
- Contact your surgeon immediately if you develop fever, increasing chest pain, or trouble breathing.
Balancing Benefits & Risks
What are the upside benefits?
When treatment is timely, the upside is huge: mortality drops from 40% to under 10%, hospital stays shrink, and most patients return to normal diets within a couple of months. Early intervention also means fewer long-term complications like strictures or chronic reflux.
What risks should you keep in mind?
Every intervention carries some risk. Surgery can lead to pain, infection, or lung complications. Stents may migrate or cause discomfort. Even conservative care isn't risk-freeif the leak isn't truly contained, infection can spread silently. The key is a balanced conversation with your doctor, weighing the severity of the tear against your overall health.
Decision-making aid
Consider printing a simple worksheet: list your symptoms, the size of the tear (once known), your comorbidities (like heart disease or diabetes), and your personal preferences (e.g., willingness for surgery). Bring this to your appointment so you and your care team can arrive at a shared decision.
Choosing the Right Team
Which credentials matter?
Look for board-certified thoracic or gastrointestinal surgeons who specialize in esophageal surgery, and gastroenterologists experienced in therapeutic endoscopy. Many high-volume centers publish their outcomesdon't be shy about asking for their esophagus tear survival rate and complication statistics.
What hospital resources are essential?
A top-tier facility will have 24-hour ICU beds, interventional radiology, and a dedicated esophageal surgery unit. For example, the team at combines surgical expertise with endoscopic capabilities, offering both minimally invasive and open options.
Patient story
Maria, 62, was diagnosed after a routine endoscopy caused a small tear. She chose a center known for its multidisciplinary esophageal team. Within two days, she had a covered stent placed, followed by a short hospital stay and a smooth transition to oral feeding. I felt like I was in the best hands, she says, and that made all the difference.
Conclusion
Facing an esophageal perforation can feel like staring down a cliff, but modern esophageal perforation treatment gives you a sturdy rope to climb back up. By recognizing the warning signs, seeking rapid diagnosis, and collaborating with an experienced medical team, you dramatically improve your chances of survival and a swift return to normal life. Remember, the sooner the leak is sealed, the sooner you'll be enjoying a hearty meal without fear.
If you or someone you love is dealing with this condition, don't waitcall emergency services the moment symptoms appear. And once you're in care, ask your doctor about the best treatment path, the expected recovery timeline, and what you can do at home to support healing. Your health journey is a team effort, and you deserve the best possible guidance.
FAQs
What are the early warning signs of an esophageal perforation?
Sudden, severe chest or neck pain, vomiting that won’t stop, fever, difficulty swallowing, sub‑cutaneous emphysema (a crackling feeling under the skin), or shortness of breath after an endoscopic procedure are classic red‑flag symptoms.
How do doctors confirm that an esophageal perforation has occurred?
The first step is usually a contrast esophagogram with water‑soluble dye. If the leak isn’t clear, a CT scan with oral contrast is performed, which shows the exact location of the tear and any associated fluid collections.
When is conservative (non‑surgical) management an option?
Conservative care is considered for small leaks (< 2 cm), well‑contained, and in patients who are hemodynamically stable. It involves nothing by mouth (NPO), broad‑spectrum IV antibiotics, close monitoring, and drainage of any collections.
What does endoscopic stent placement entail and how long does the stent stay in place?
A self‑expanding metal or plastic stent is deployed across the tear under endoscopic guidance, sealing the hole while the tissue heals. Stents are typically left for 4–8 weeks, after which they are endoscopically removed.
What should a patient expect during the recovery period after treatment?
Hospital stay is usually 5–10 days for monitoring and antibiotics. Nutrition is provided intravenously or via a feeding tube until oral intake is safe. Full diet is often resumed 6–8 weeks after surgical repair, 4–8 weeks after stenting, and 2–3 weeks after conservative care. Follow‑up endoscopy, a gradual diet advance, and lifestyle modifications (e.g., no smoking) are essential to prevent strictures or recurrence.