Quick answer: adrenal masses show up in roughly 5%7% of adults on routine imaging, and the odds climb as we get older. Most of them are harmless, but a small slice can cause hormone problems or turn malignantso knowing how common they are helps you and your doctor decide how aggressively to investigate.
Why does it matter? Because the difference between watching a tiny incidentaloma and rushing to surgery can feel like walking a tightrope. This guide breaks down the numbers, the red flags, the workup steps, and what treatment looks likeso you can feel confident about the next step.
Adrenal Mass Epidemiology
When you hear adrenal mass, you might picture a rare tumor lurking in a secret corner of your body. In reality, it's more like that unexpected third cousin who shows up at a family reunioncommon enough to be noteworthy, but most of the time, they're just passing through.
Large imaging studies from the United States and Europe have consistently reported an overall prevalence of about 57% in the general adult population. The rate jumps to 1012% in people over 70, according to a recent populationbased review. In younger adults (under 40), the prevalence drops to roughly 12%, so age is a key driver.
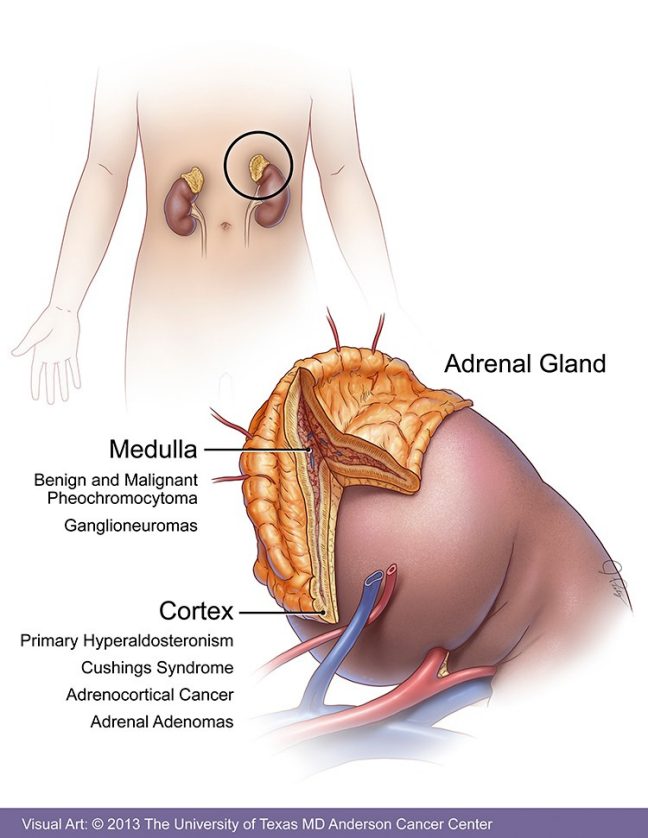
What kinds of lesions are we talking about? The vast majority (8085%) are nonfunctioning adenomastiny, lipidrich nodules that don't secrete hormones. The rest are split between functional adenomas (producing excess cortisol, aldosterone, or androgens), pheochromocytomas (catecholaminesecreting tumors), and the far rarer adrenocortical carcinoma (ACC).
| Age Group | Prevalence of Adrenal Mass |
|---|---|
| <40 years | 12% |
| 4065 years | 57% |
| >65 years | 1012% |
Clinical Importance Highlights
Finding an incidental adrenal lesion can feel like a "what now?" moment. Most of the time, there's nothing to worry about, but a handful of features should light up a red flag.
- Size matters. Lesions 4 cm have a higher chance of being malignant.
- Hormone excess. Unexplained high blood pressure, rapid weight gain, or low potassium could point to a functional adenoma.
- Imaging characteristics. Hounsfield units (HU) >10 on noncontrast CT, irregular borders, or rapid growth raise suspicion.
How often does a mass turn out to be cancer? Adrenocortical carcinoma accounts for less than 0.2% of all adrenal lesions, but its impact is outsized. Reports show a 5year survival rate of roughly 30% for localized disease, dropping below 10% once it spreads.
Symptoms of a functional adrenal adenoma can be subtle: occasional headaches, mild hypertension, or a slight swelling of the faceoften dismissed as stress. That's why a thorough workup is essential.
Standard Workup Algorithm
Imagine you're a detective with a new clue (the mass) and a toolbox (labs, imaging). Here's the stepbystep adrenal mass workup algorithm most endocrinologists follow.
- Initial labs (adrenal mass workup labs). Start with:
- Plasma or urinary metanephrines (screen for pheochromocytoma).
- Overnight 1 mg dexamethasone suppression test (check for autonomous cortisol production).
- Aldosterone/renin ratio (if the patient is hypertensive or has hypokalemia).
- Imaging review. Noncontrast CT is firstline. If the lesion is lipidrich (HU 10), chances are it's a benign adenoma. Otherwise, consider MRI with chemical shift imaging or 18FFDG PET for metabolic activity.
- Decision node. Based on size, lab results, and imaging:
- Observation (repeat imaging in 612 months) for <1 cm or stable <4 cm nonfunctioning lesions.
- Endocrine referral and possible surgery for 4 cm, hormonal excess, or suspicious imaging.
This algorithm balances the need to catch dangerous tumors early while sparing patients from unnecessary surgery.
Adenoma vs Pheochromocytoma
Both adenomas and pheochromocytomas sit in the adrenal gland, but their personalities are worlds apart.
Imaging clues: Adenomas are usually homogeneous, have low HU values, and lose signal on outofphase MRI (thanks to intracellular fat). Pheochromocytomas, on the other hand, are often hypervascular, have higher HU, and may show a lightbulbbright T2 signal on MRI.
Hormone tests: Metanephrines soar in pheochromocytoma, while cortisol, aldosterone, or androgen levels may be abnormal in functional adenomas. A negative metanephrine test combined with low HU points strongly toward a benign adenoma.
Missing a pheochromocytoma can be dangeroussurprise surgery could trigger a hypertensive crisis. That's why the workup labs are nonnegotiable.
Size Criteria Guidance
Size is the most straightforward but also the most debated factor. Here's a quick cheatsheet that many guidelines reference:
| Lesion Size | Recommended Management |
|---|---|
| <1 cm | Observation; repeat imaging in 12 months if stable |
| 14 cm | Consider labs; if nonfunctioning and benign imaging observe; if functional or suspicious refer for surgery |
| >4 cm | Strong recommendation for surgical removal (laparoscopic or open) |
Why isn't size alone enough? Some small lesions (<2 cm) can be hormonally active, while a few larger ones may still be benign. That's why the adrenal adenoma size criteria must be paired with lab results and imaging features.
Treatment Options Explained
Once a decision for surgery is madeor if a functional adenoma needs medical controlthe options branch out.
- Medical management. For cortisolproducing adenomas, ketoconazole or metyrapone can control excess hormones before surgery. Aldosteroneproducing lesions may need mineralocorticoid receptor antagonists (spironolactone, eplerenone) while awaiting definitive treatment.
- Surgical approaches. Laparoscopic adrenalectomy is the gold standard for most benign lesions, offering quicker recovery and less pain. Robotic platforms add precision, especially for large or posterior tumors. Open adrenalectomy is reserved for suspected ACC or very large masses.
- Postoperative followup. Hormone levels are checked at 1 month and 6 months postop. Imaging is repeated at 6 months for adenomas and annually for any borderline lesions.
Choosing between surgery and medication isn't just a medical decisionit's a personal one. Discuss lifestyle, comorbidities, and recovery expectations openly with your doctor.
Prognosis & Survival
If the final diagnosis is a benign adenoma, the prognosis is essentially excellentmost people live normal lives without further intervention.
For adrenocortical carcinoma, the picture is sobering. The adrenocortical carcinoma survival rate hinges on stage at diagnosis:
- Stage I (localized): 5year survival 6070%.
- Stage II (larger tumor, still localized): 5year survival 4050%.
- Stage III/IV (regional spread or metastasis): 5year survival drops below 10%.
The death rate for adrenal cancer remains low in absolute numbersabout 12 per 100,000but the aggressive nature of ACC makes early detection crucial. Multidisciplinary care, including surgery, adjuvant mitotane, and sometimes radiation, offers the best chance.
Patient Stories & Cases
Case A The Silent Spotter. Maria, 52, was getting a CT scan for kidney stones when radiology reported a 1.2 cm left adrenal nodule. Labs were normal, the lesion had low HU, and it stayed the same size after a year. She's been living symptomfree, and her doctor simply monitors it every 23 years.
Case B The Unexpected Surge. James, 38, presented with episodic pounding headaches and sweating. An MRI revealed a 2.8 cm adrenal mass with high T2 signal. Metanephrine levels were skyhigh, confirming pheochromocytoma. He underwent laparoscopic removal, and his episodes vanished. "I felt like a flashbang went off in my head," James joked, grateful for the quick fix.
Case C The Large Mystery. Linda, 66, had a 5.5 cm adrenal mass discovered on a routine chest CT. Hormone workup was negative, but the size and irregular borders prompted surgery. Pathology revealed adrenocortical carcinoma confined to the gland. She now follows a rigorous surveillance schedule and has embraced a supportive community of fellow survivors.
These stories illustrate the spectrumfrom watchful waiting to urgent surgeryhighlighting why personalized evaluation matters. If you'd like reading on related endocrine and metabolic topics, see an overview on adrenal tumor size for more on how size affects management.
Trusted Sources & Links
For anyone craving deeper dives, the following resources are solid pillars of evidence:
- Endocrine Society Clinical Practice Guidelines (2023) comprehensive recommendations for adrenal incidentalomas.
- American Association of Clinical Endocrinologists (AACE) consensus statements on adrenal mass workup.
- National Cancer Institute (NCI) ACC data page uptodate survival statistics and treatment advances.
- Peerreviewed studies on adrenal mass prevalence and imaging criteria.
All these references are vetted by specialists, ensuring the information you read here stands on a reliable foundation.
Conclusion
Adrenal mass prevalence is surprisingly highespecially as we agebut the good news is that most of these lesions are benign and harmless. By understanding the size criteria, the hormonal workup labs, and the imaging clues, you can partner with your physician to make smart, balanced decisions. Whether it's simply observing a tiny, nonfunctioning nodule or taking decisive action against a hormonesecreting tumor, you're not alone. If you've found an incidentaloma, talk openly with your doctor, ask questions, and consider sharing your experience in the comments. Your story might just help the next person navigating the same uncertain road.
FAQs
What is the prevalence of adrenal masses in adults?
Adrenal masses are found in about 5–7% of adults on routine imaging, with rates increasing to 10–12% in those over 65 years old.
Are most adrenal masses benign?
Yes, the majority of adrenal masses are benign non-functioning adenomas, with only a small percentage being malignant or hormone-producing.
How is an adrenal mass diagnosed?
Adrenal masses are usually detected incidentally on imaging like CT or MRI, followed by lab tests to check for hormone excess and further imaging if needed.
When should an adrenal mass be treated?
Treatment is considered for masses larger than 4 cm, those with suspicious imaging features, or if there is evidence of hormone excess or malignancy.
What are the symptoms of a functional adrenal mass?
Symptoms may include high blood pressure, rapid weight gain, low potassium, or episodic headaches, depending on the hormones produced by the mass.