Most people who hear adrenal tumor panic is it cancer? Will I need surgery? The short answer is that the majority of adrenal tumors are harmlessbenign adenomas, and only a small slice turn out to be cancerous. Knowing the exact type is the key to deciding whether you simply watch, treat hormones, or head straight to the operating room.
Lets walk through the different adrenal tumor types together, explore the symptoms you might notice (especially if youre a woman), and figure out the best next steps. Im here to keep the medical jargon light, share a few realworld stories, and give you the confidence to ask the right questions at your next doctors visit.
Overview of Types
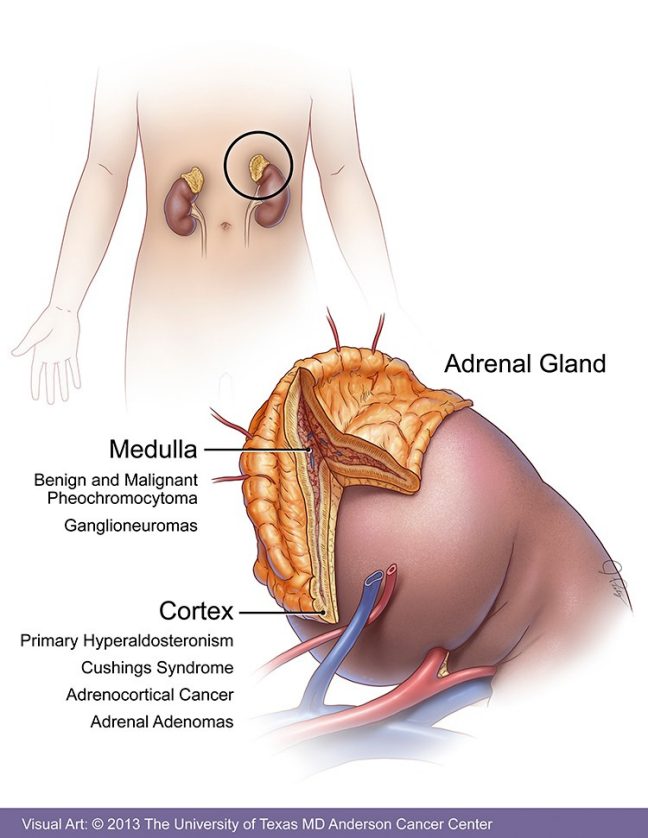
The adrenal glands sit right on top of each kidney, split into two zones the cortex (which makes steroids) and the medulla (which pumps out adrenaline). Tumors can arise from either zone and fall into two broad camps: benign and malignant. Below is a quick sidebyside look.
| Feature | Benign Tumors | Malignant Tumors |
|---|---|---|
| Typical size | Usually <4cm | Often >4cm, may grow fast |
| Hormone production | Can be functional (e.g., aldosterone, cortisol) | May overproduce cortisol, androgens, or catecholamines |
| Imaging clues | Smooth borders, homogeneous | Irregular shape, necrosis, local invasion |
| Treatment | Surveillance or simple surgery | Surgery+adjuvant therapy (mitotane, chemo, clinical trials) |
According to the , only about 510% of adrenal tumors are malignant. Thats reassuring, but it also means we cant ignore a lump that shows worrisome features.
Benign Tumor Symptoms
Even benign doesnt always mean no symptoms. Some harmlesslooking tumors secrete hormones that tip the bodys balance.
Adenoma (Incidentaloma)
Most adenomas are discovered incidentally on a CT scan done for something else hence the nickname incidentaloma. If theyre nonfunctional, you might never notice them. But a functional adenoma can cause:
- High blood pressure
- Fatigue or weight gain (if it makes extra cortisol)
- Mild electrolyte changes
Aldosteronoma (Conns Syndrome)
These tumors overproduce aldosterone, leading to saltyspotted symptoms. In women, you might feel:
- Headaches that wont quit
- Muscle cramps or pins and needles
- Unexplained swelling in hands or feet
Pheochromocytoma (Usually Benign)
Even though pheochromocytomas can be scary, the majority are benign. They release bursts of adrenaline, giving you the classic triad:
- Sudden pounding headache
- Profuse sweating
- Rapid heartbeat or palpitations
AndrogenSecreting Tumors in Females
When a tumor decides to crank out male hormones, women notice:
- Unwanted facial or body hair (hirsutism)
- Acne that wont clear up
- Irregular periods or even missed cycles
- Deepening voice over time
Quick Symptom Checklist for Women
Check any of these boxes if youre feeling off and have an adrenal finding on imaging:
- Persistent high blood pressure
- Unexplained weight changes
- New facial hair or acne
- Frequent headaches with sweating
- Irregular menstrual bleeding
Malignant Tumor Signs
Malignant adrenal tumors are less common but far more aggressive. The two big players are adrenocortical carcinoma (ACC) and metastatic lesions that spread from cancers elsewhere.
Adrenocortical Carcinoma (ACC)
ACC can grow rapidly studies show a median doubling time of 36months. Early signs often masquerade as benign hormone excess, but by the time the tumor reaches stage4, symptoms may include:
- Severe abdominal or flank pain
- Unintentional weight loss and loss of appetite
- Jaundice or liver tenderness (if it spreads to the liver)
- Bone pain or fractures (bone metastases)
Metastatic Lesions to the Adrenal Gland
Common primary cancers that love to set up camp in the adrenal glands include lung, breast, melanoma, and renal cell carcinoma. Symptoms usually mirror the original cancers behavior often painless enlargement discovered on imaging.
Malignant Pheochromocytoma / Paraganglioma
These rare beasts cause extreme spikes in blood pressure, sometimes leading to hypertensive crises think headache so bad I cant see and sweating that drenches your shirt within minutes.
GrowthRate Visual Guide
Below is a simple chart that shows typical growth per month for benign vs malignant adrenal lesions.
| Tumor Type | Average Monthly Growth |
|---|---|
| Benign Adenoma | 0.10.3cm |
| ACC | 0.51.0cm (or more) |
| Metastatic Lesion | Variable, often rapid |
Diagnosis Steps
When your doctor spots an adrenal mass, the next few weeks become a detective story. Heres the usual script:
Imaging
- CT scan First line, looks at size, density, and washout characteristics (a quick blush of contrast that fades tells you a lot).
- MRI Helpful for characterizing tissue composition, especially if you suspect a pheochromocytoma.
- PET scan Used when cancer spread is a concern.
Hormone Workup
Blood and urine tests check for excess hormones:
- Plasma metanephrines and catecholamines (pheochromocytoma screen).
- Aldosteronetorenin ratio (Conns syndrome).
- Overnight dexamethasone suppression test (Cushings syndrome).
- Serum DHEASulfate (androgensecreting tumors).
Biopsy When and Why
Biopsies of adrenal masses are risky because of possible bleeding and catecholamine surge. Theyre usually reserved for cases where imaging and labs cant tell if the tumor is metastatic.
Expert Tip
Endocrinology specialists often look at the CT washout curve. A rapid washout (more than 60% within 10 minutes) strongly points to a benign adenoma a nugget of wisdom you can ask your doctor about.
Treatment Options
Treatment splits cleanly along the benignvsmalignant line, but there are nuances based on size, function, and patient health.
Benign Tumors Watchful Waiting or Surgery
Guidelines say if a nonfunctional tumor is under 4cm and looks smooth on imaging, you can monitor it with an annual CT or MRI. If it grows, becomes functional, or worries you, laparoscopic adrenalectomy is a safe, minimally invasive option.
Functional Benign Tumors HormoneTargeted Therapy
- Aldosteronoma: Mineralocorticoid receptor antagonists like spironolactone help control blood pressure while you decide on surgery.
- Pheochromocytoma: Alphablockers (phenoxybenzamine) are started weeks before surgery to prevent dangerous spikes during the operation.
Malignant Tumors Multimodal Attack
Adrenocortical carcinoma usually needs an outright surgical removal (if its resectable) followed by adjuvant therapy. The standard drug is mitotane, sometimes combined with platinumbased chemotherapy. In recent years, clinical trials have explored immune checkpoint inhibitors like pembrolizumab a promising avenue for patients with advanced disease.
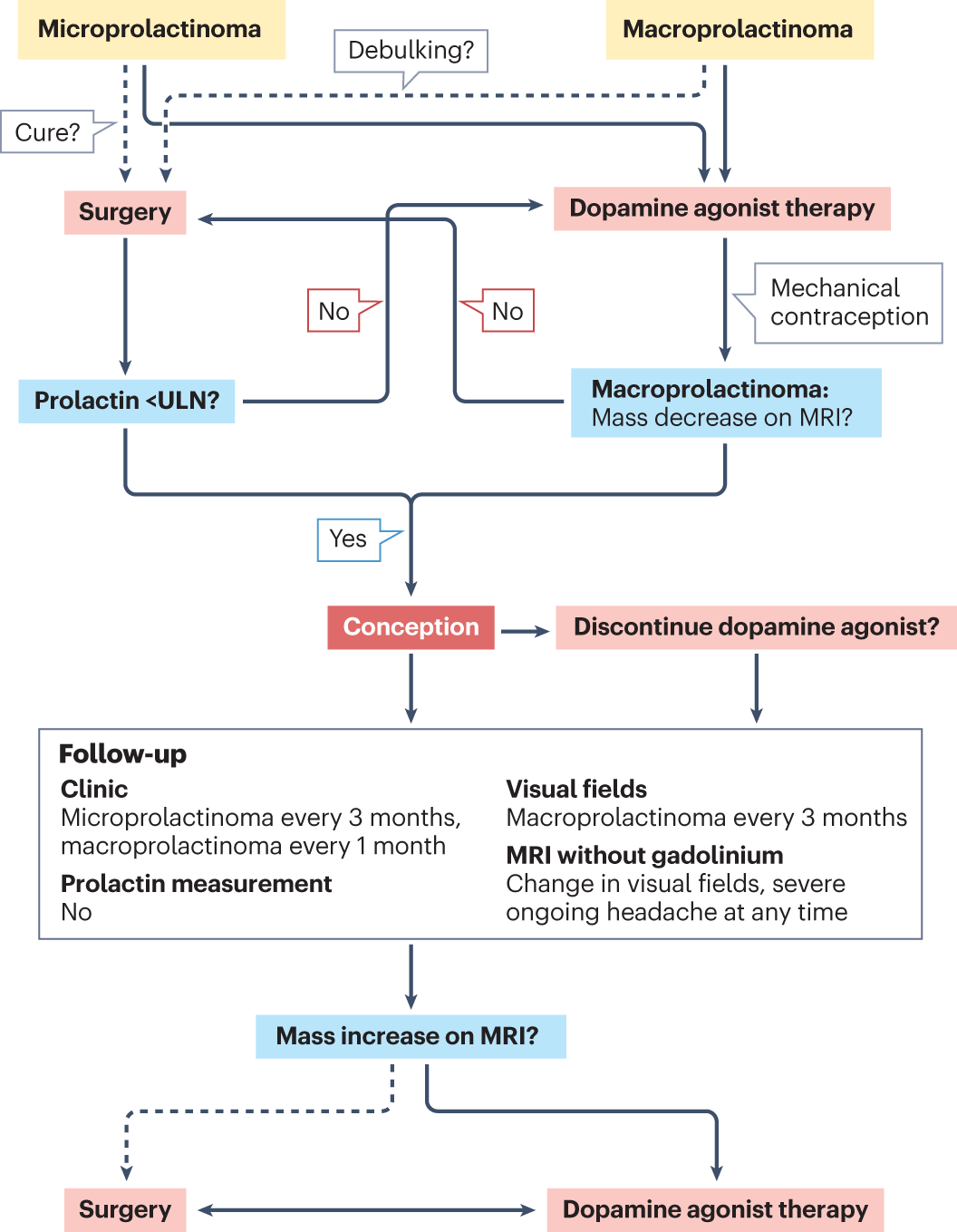
DecisionTree Flowchart (Treatment Algorithm)
Imagine a flowchart that starts with Is the tumor >4cm or functional? Yes Biochemical testing If malignant suspicion Refer to surgical oncology Postop adjuvant therapy. If No, the path leads to Surveillance every 612months. Visualizing this helps you ask the right questions during followup.
Living with an Adrenal Tumor
Beyond the medical checklist, theres a daytoday side of the story. Here are some practical tips that have helped people Ive spoken with.
How Fast Do Adrenal Tumors Grow?
Benign adenomas usually crawl along at a snails pace a few millimeters a year. Malignant ACC, on the other hand, can sprint a centimeter or more in just a couple of months. Knowing the growth rate can ease anxiety (slow growth = less urgency) or prompt quicker action (rapid growth = worry).
Can a Benign Tumor Cause Serious Problems?
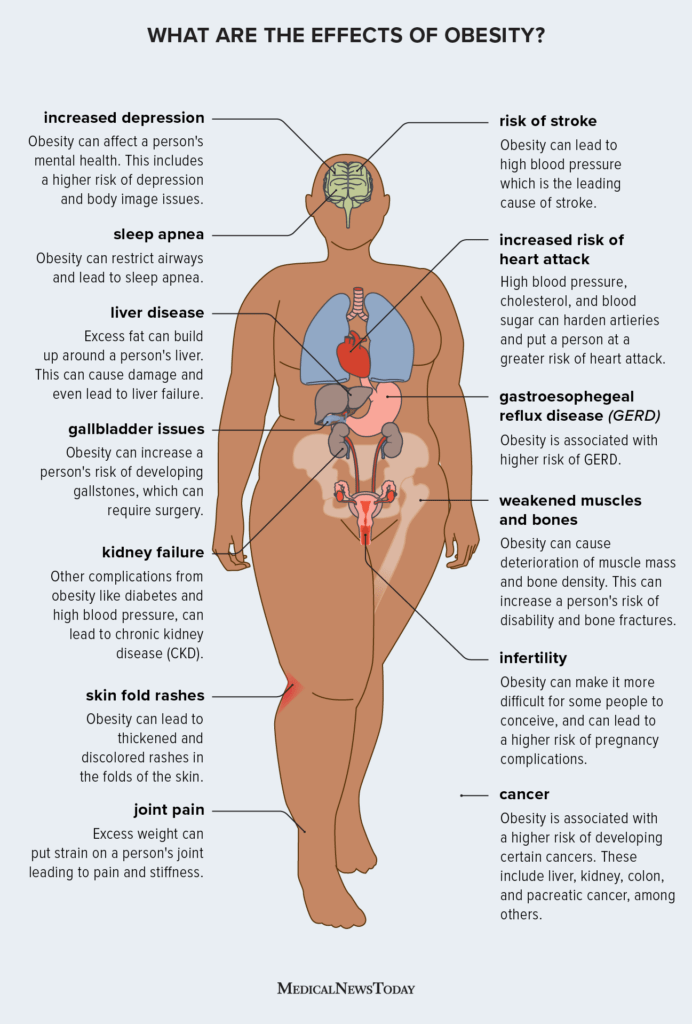
Yes, if it secretes hormones. A quiet tumor that makes excess cortisol can lead to Cushings syndrome think moonface, thinning skin, and easy bruising. Thats why hormone panels are a must, even for a benign label. If you notice weight changes concentrated around the trunk (similar to truncal obesity), mention that specifically to your clinician it can be a clue to cortisol excess and may prompt focused testing or referral for truncal obesity evaluation and management.
FollowUp Schedule You Can Trust
Most endocrinologists recommend a repeat CT or MRI at 612months after the initial discovery, then yearly if nothing changes. If youre on medication to control hormone excess, labs are checked every 36months.
PatientStory Box (Experience)
Sarah, a 38yearold teacher, found out she had a 2.5cm adrenal incidentaloma after a CT for a sinus infection. She felt fine, but a few weeks later she noticed new hair growth on her chin and irregular periods. Blood work revealed elevated DHEASulfate an androgensecreting tumor. After a laparoscopic adrenalectomy, her hormones normalized, and shes back to running marathons. Sarah says the biggest relief was having a doctor who actually explained what each test meant, instead of throwing medical jargon at me.
TakeHome Messages
Understanding adrenal tumor types is empowering. Most are benign adenomas that require simple monitoring, while a tiny fraction are aggressive cancers that need prompt, aggressive treatment. Hormoneproducing tumors can cause real symptoms, especially in women, so never ignore persistent high blood pressure, unexplained hair growth, or sudden headaches.
If youve been told you have an adrenal mass, ask your doctor about:
- Size and imaging characteristics (smooth vs irregular)
- Hormone panel results (are any hormones high?)
- Growth rate on followup scans
- Whether a surgical referral is warranted
Remember, youre not alone on this journey many have walked the path, asked the same questions, and emerged with clear plans. If you have more questions, feel free to share your experience in the comments or reach out to a qualified endocrinologist. Your health deserves clarity, compassion, and a little bit of friendly guidance.
FAQs
What are the most common benign adrenal tumor types?
The most frequent benign lesions are adrenal adenomas (often found incidentally) and functional tumors such as aldosteronomas, cortisol‑producing adenomas, and pheochromocytomas.
How can I tell if an adrenal tumor is malignant?
Malignant features include size greater than 4 cm, rapid growth (often >0.5 cm/month), irregular borders, necrosis on imaging, and hormone excess that is aggressive or unusual.
Which symptoms should make a woman suspect a hormone‑secreting adrenal tumor?
Look for high blood pressure, unexplained weight changes, new facial or body hair (hirsutism), persistent acne, irregular menstrual cycles, sudden headaches with sweating, or muscle cramps.
What tests are used to diagnose adrenal tumor types?
Diagnosis usually starts with a CT or MRI to assess size and appearance, followed by hormone panels: plasma metanephrines, aldosterone‑renin ratio, dexamethasone suppression test, and DHEA‑Sulfate levels.
When is surgery recommended for an adrenal tumor?
Surgery is advised if the tumor is larger than 4 cm, shows suspicious malignant characteristics, is functional (hormone‑producing), or if it grows on follow‑up imaging.