Finding a spot on a scan that you didnt know was there can feel like stepping onto a shaky bridge youre not sure whether to keep moving or turn back. The good news? Most adrenal nodules are harmless, and size is the most useful clue doctors have to decide what comes next. In a nutshell, the larger the adrenal tumor size, the higher the chance it could be a problem, but many small lesions never cause trouble at all.
In the next few minutes well walk through exactly what an adrenal tumor is, how size categories translate into risk, how fast these growths usually move, what symptoms (if any) you might notice, and which treatment paths make sense. Think of this as a friendly coffeechat about a topic that can feel heavy, but doesnt have to be confusing.
Adrenal Tumor Basics
Definition: Incidentaloma, Adenoma, Carcinoma
An adrenal incidentaloma is a fancy term for a mass thats discovered by accident most often during a CT or MRI done for something else. The majority are adenomas, which are benign (noncancerous) growths. A tiny fraction turn out to be malignant (cancerous) adrenal carcinomas, and even fewer are functional tumors that secrete hormones.
How Common Are They?
Studies show that up to 9% of adults have an adrenal lesion larger than 0.5cm when scanned for unrelated reasons. When the cutoff rises to 1cm, the prevalence drops to around 3%. So yes, finding a nodule isnt as rare as you might think.
Why Size Matters
Think of size as the first checkpoint on a road map. It tells doctors whether the journey ahead will likely be a quick stroll (just watchful waiting) or a longer trek that may need surgery. Thats why the phrase adrenal tumor size shows up in every guideline.
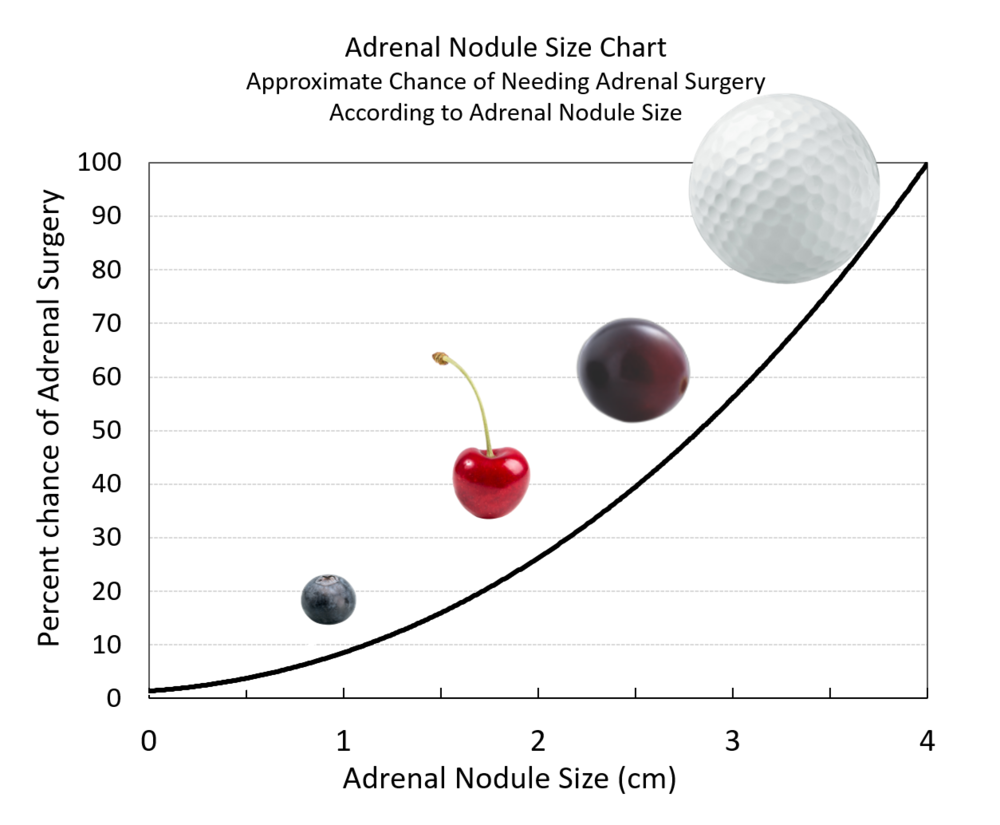
Size Categories & Risk
Less Than 1cm
These tiny spots, often measured as 10mm or less, are usually benign. A 10mm left adrenal nodule, for example, rarely causes problems and most doctors recommend a repeat scan in a year just to confirm its staying put.
12cm (Including 1cm Nodule on Adrenal Gland)
This is the sweet spot where most incidentalomas sit. About 3% of nodules in this range turn out to be malignant. Because the risk is low, regular monitoring (often every 612 months) is the norm, unless the nodule is hormonally active.
24cm (Think 2cm Nodule on Adrenal Gland)
Here the concern nudges up a bit. Roughly 57% of lesions in this bracket are cancerous. Doctors may still opt for surveillance, especially if imaging features look benign, but the conversation about surgery becomes more common.
46cm
Risk rises to about 710%. Many endocrinologists recommend a CTguided biopsy or surgical removal, particularly if the tumor is growing or causing hormonal symptoms.
Greater Than 6cm
This is the red zone. The odds of malignancy jump significantly, sometimes exceeding 20%. Most guidelines suggest surgical excision unless the patient is a highrisk surgical candidate.
| Size Range | Estimated Cancer Risk | Typical Management | Key References |
|---|---|---|---|
| 1cm (10mm) | 12% | Annual imaging, no immediate surgery | |
| 12cm | 3% | 612month imaging; hormone testing | |
| 24cm | 57% | Consider surgery if rapid growth or functional | |
| 46cm | 710% | Biopsy or surgical removal recommended | |
| >6cm | >20% | Strong recommendation for surgery |
Tumor Growth Speed
Average Growth Rates
About 20% of lesions 1cm show measurable growth over a fiveyear span, typically less than 0.5cm per year. Thats like a snails pace on a marathon track not urgent, but worth watching.
Factors Influencing Growth
Age, underlying genetic syndromes (like MEN1), and whether the tumor secretes hormones can all speed up growth. For example, cortisolproducing adenomas sometimes enlarge faster than nonfunctional ones.
Monitoring Schedule
Most experts recommend a baseline scan, then a followup at 612months. If the nodule stays the same size, the interval can stretch to 23years. However, any increase >0.5cm per year usually triggers a more aggressive workup.
Symptoms and Concerns
Typical (or Absent) Symptoms of Benign Nodules
Heres the reassuring part: many people never feel anything. Benign adrenal lesions often sit quietly, discovered only because you got a scan for an unrelated issue.
RedFlag Symptoms
If the nodule is functional, you might notice:
- High blood pressure that wont calm down.
- Sudden weight gain, especially around the face and neck.
- Muscle weakness or frequent fatigue.
- Unexplained palpitations or sweating.
These signs suggest hormone overproduction, and theyre a cue to bring the nodule to your doctors attention right away.
Should I Be Worried About a Nodule on My Adrenal Gland?
Short answer: it depends on size and symptoms. A 1cm nodule thats stable and nonfunctional is usually lowrisk. A 4cm growth thats causing high blood pressure, however, warrants prompt evaluation.
Personal Story
Let me share a quick anecdote. My friend Maya, 45, had a routine CT for a kidney stone. The radiologist flagged a 2cm adrenal nodule. Naturally, Maya panicked. Her endocrinologist ordered hormone panels and a repeat CT after 6 months. The nodule didnt change, and hormone levels were normal. Mayas story ends with a just watch plan and a lot less anxiety. Its a reminder that numbers on a screen rarely dictate destiny without context.
Treatment Options Overview
Observation & Surveillance
For most nodules under 4cm, especially when theyre nonfunctional, the gold standard is watchful waiting. This means periodic imaging and hormone testing, but no surgery.
Surgical Removal
When size crosses the 4cm threshold, or when the tumor grows quickly or secretes hormones, a surgeon may recommend an adrenalectomy. Laparoscopic (keyhole) surgery is now the norm, offering quicker recovery and less pain than open surgery.
Minimally Invasive Techniques
Robotic adrenalectomy is gaining popularity in highvolume centers. The robots precision can make it easier to dissect around vital blood vessels, especially for larger tumors.
Hormonal Therapy for Functional Tumors
If a tumor is producing excess cortisol, aldosterone, or catecholamines, medication can help control those hormones while you decide on surgery. For example, metyrapone can blunt cortisol production temporarily.
DecisionMaking Checklist
- Size of the lesion (1cm, 12cm, 24cm, >4cm).
- Growth rate on serial imaging.
- Hormonal activity (yes/no, which hormone?).
- Patients age, overall health, and surgical risk.
- Patient preference after understanding risks and benefits.
RealWorld Experience Stories
CaseStudy 1: The 1cm Surprise
A 30yearold marathon runner had a CT for a foot injury. A 1cm left adrenal nodule showed up. Hormone workup was negative, and the nodule stayed the same size for three years. He kept training, and the nodule never caused trouble.
CaseStudy 2: 3cm Functional Tumor
Emily, 52, presented with resistant hypertension. Imaging revealed a 3cm adrenal mass. Lab tests showed excess aldosterone. After a brief course of spironolactone, she opted for laparoscopic removal. Postop, her blood pressure normalized, and she stopped her antihypertensives.
Expert Insight
Dr. Patel, an endocrine surgeon at a major academic center, explains, We never make a decision based on size alone. The contexthormones, growth, patient healthshapes the plan. Thats why a multidisciplinary discussion is key. (source: ).
Bottom Line Summary
In the world of adrenal nodules, size is the compass, not the final destination. Small nodules (1cm) are almost always benign and can be safely observed. As the adrenal tumor size climbs into the 24cm range, the risk creeps up, but many still remain noncancerous and are managed with regular scans. Anything larger than 4cm, especially if its growing or secreting hormones, usually calls for surgical consideration.
Remember, youre not alone on this journey. Real patients like Maya, Emily, and countless others have walked the same path, sharing both worries and relief. If youve discovered an adrenal nodule, talk openly with your doctor about size, hormone tests, and the followup schedule that feels right for you. Keep the conversation going, track any new symptoms, and trust that the combination of expertise and personal experience will guide you to the best decision.
Whats your experience with adrenal incidental findings? Have you found a plan that worked for you? Feel free to share in the comments or ask any questionsyoure part of a supportive community thats here to help.
For readers also managing metabolic concerns, simple dietary choices can matter for example, small studies suggest foods like strawberries blood sugar responses may be more favorable than higherglycemic fruits, which can be useful context when addressing weight changes that sometimes accompany hormonal disorders.