Yes, certain gene mutations can cause a special form of diabetes called monogenic diabetes (often referred to as MODY). It's not the same as type 1 or type 2, and it usually runs in families.
In the next few minutes we'll walk through which genes are involved, how you can recognize the signs, whether a genetic test makes sense, and what treatment options are availableso you can decide if you or a loved one should explore genetic testing.
Why Gene Mutations Matter
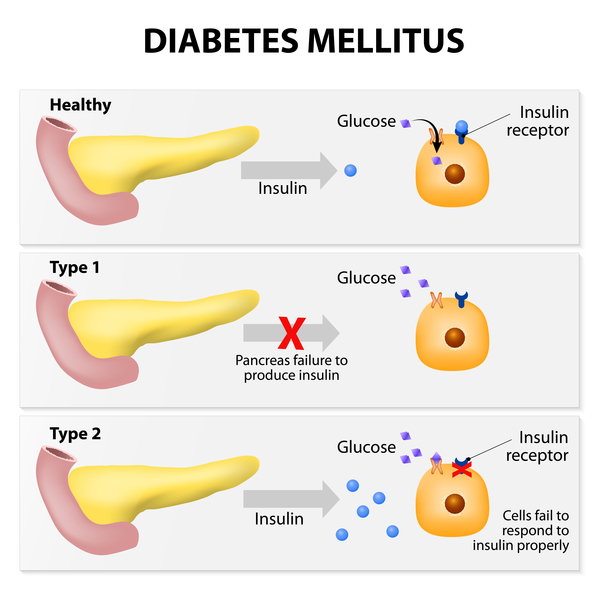
When most people think about diabetes, they picture the classic narratives of type 1 (autoimmune) or type 2 (lifestyle-related). Those stories focus on many genes working together with diet, exercise, and the environment. Gene mutation diabetes, however, tells a very different story: a single genetic change can be enough to alter how your pancreas makes insulin.
Monogenic diabetes, technically called MODY (Maturity-Onset Diabetes of the Young), accounts for roughly 12% of all diabetes cases. The difference matters because the treatment, prognosis, and even the emotional impact can be completely distinct from the more common forms.
What type of mutation causes diabetes?
Most MODY-related mutations are missense or nonsense changes that affect a single amino acid in a protein crucial for beta-cell function. Some are splice-site alterations that disrupt how the gene's message is assembled, and a few affect promoter regions that control how much of the protein is made.
Take the GCK gene, for example. A single-point missense mutation in GCK reduces the enzyme's ability to sense glucose, leading to a mild, often asymptomatic elevation of blood sugar. This is the classic cause of MODY2, and you can read more about it in the .
Mini-case study GCK-MODY2
Emma, a 28-year-old graphic designer, was told she had prediabetes after a routine checkup showed a fasting glucose of 108 mg/dL. She felt fine, exercised regularly, and had no family history of type 1 diabetes. A genetic panel revealed a GCK missense mutation. With this knowledge, her doctor explained that intensive medication wasn't neededjust yearly monitoring.
Which genes are most commonly linked to monogenic diabetes?
| Gene | Common MODY Type | Key Feature |
|---|---|---|
| GCK | MODY2 | Mild fasting hyperglycemia, often no treatment needed |
| HNF1A | MODY3 | Responsive to low-dose sulfonylureas |
| HNF4A | MODY1 | Similar to HNF1A, sometimes neonatal macrosomia |
| HNF1B | MODY5 | Often associated with kidney anomalies |
| INS | MODY10 | Rare, insulin deficiency from birth |
These five genes account for the majority of MODY diagnoses. Each brings its own clinical phenotype, which is why a precise genetic test can be a game-changer.
How do these mutations differ from the genetics of type 1 & type 2?
Type 1 diabetes is largely polygenic, with the strongest risk coming from the HLA region (especially HLA-DR and HLA-DQ alleles) combined with other loci like INS and CTLA4. Environmental triggersviral infections, early-life dietplay a big role too. By contrast, MODY is typically a single-gene defect with high penetrance, meaning if you inherit the mutation you'll almost certainly develop the condition.
Type 2 diabetes involves dozens, if not hundreds, of genes that each nudge your risk a little higher. Lifestyle factors frequently tip the scale. In short, MODY is the "one-hit" wonder of diabetes genetics, while type 1 and type 2 are more like a whole orchestra playing together.
Spotting the Signs
One of the most frustrating parts of MODY is that its symptoms often masquerade as either early-onset type 1 or a very mild type 2. Knowing what to look for can save monthsor even yearsof unnecessary treatment.
What are the main MODY diabetes symptoms?
- Onset before age 25, often in the late teens or early twenties.
- Persistent mild hyperglycemia (fasting glucose 100130 mg/dL) without classic type 1 signs like ketoacidosis.
- Stable A1C that hovers around 67% over many years.
- Negative diabetes-related autoantibodies (GAD, IA-2, ZnT8).
- Strong multigenerational patternusually a parent and several children are affected.
These clues are subtle, which is why clinicians sometimes label the condition "atypical type 1" or "early-onset type 2."
MODY vs. Type 1 Diabetes How to tell?
| Feature | MODY | Type 1 Diabetes |
|---|---|---|
| Age at onset | Usually <25y | Any age, peaks at 46y & 1418y |
| Autoantibodies | Negative | Positive (GAD, IA-2, ZnT8) |
| C-peptide | Normal or mildly reduced | Very low or undetectable |
| Family history | Vertical, 3+ generations | Often sporadic, though HLA risk runs in families |
| Treatment | Oral sulfonylureas or diet | Insulin from diagnosis |
If you tick more boxes on the MODY side, it's worth chatting with your doctor about a genetic test.
When should you suspect a genetic cause?
Consider a genetic evaluation when you notice any of the following:
- You were diagnosed with diabetes before 25 years old, but your labs don't look "type 1-ish."
- Several close relatives have diabetes, yet none have required insulin.
- Your doctor mentions "atypical diabetes" or you're on a low dose of sulfonylurea and it works surprisingly well.
- You have a normal C-peptide level despite years of hyperglycemia.
Getting Tested
Genetic testing for diabetes is no longer the stuff of science-fiction labs. Today's commercial panels can screen for all known MODY genes in a single blood draw, and many insurance plans cover the cost when clinical criteria are met.
How does a genetic test for diabetes work?
Typically, a phlebotomist draws a few milliliters of blood. The sample is sent to a certified laboratory where next-generation sequencing (NGS) reads the DNA code of the targeted genes. Bioinformaticians then compare your sequence to reference genomes, flagging any pathogenic variants.
Step-by-step guide to ordering a test
- Schedule an appointment with an endocrinologist or a genetics counselor.
- Discuss your personal and family history; bring any previous lab reports.
- Ask for a referral to a reputable MODY panel (e.g., ).
- Provide a blood samplemost labs need only one visit.
- Review results with a qualified professional; they'll explain whether you have a pathogenic mutation, a variant of uncertain significance (VUS), or a negative result.
Who should get tested?
Guidelines suggest testing people who meet at least two of the following:
- Diagnosis of diabetes before age 25.
- Three or more consecutive generations with diabetes, especially if treatment patterns vary.
- Negative autoantibodies but persistent hyperglycemia.
- Excellent response to a low dose of sulfonylureas despite no prior insulin use.
What do test results mean?
A positive result confirms the specific MODY subtype, guiding treatment and informing family members. A variant of uncertain significance (VUS) means the lab found a change, but its impact isn't clearhere a genetics counselor can help weigh the evidence. A negative result doesn't rule out all monogenic forms; rare undiscovered genes or technical limitations could be at play.
Treatment Options
Knowing the exact gene mutation turns the treatment decision from guesswork into a precise prescription.
What is the standard MODY diabetes treatment?
Each MODY subtype has a preferred therapeutic approach:
- MODY2 (GCK): Most people need no medicationjust lifestyle monitoring.
- MODY3 (HNF1A) & MODY1 (HNF4A): Low-dose sulfonylureas (e.g., glipizide) often achieve excellent control, sometimes better than metformin.
- MODY5 (HNF1B): Frequently requires insulin because kidney involvement can affect drug clearance.
- INS-related MODY: May need early insulin therapy, similar to type 1.
Because the response is so gene-specific, a misdiagnosis can lead to overtreatment (unnecessary insulin) or undertreatment (missing a life-saving sulfonylurea).
Treatment algorithm flowchart (suggested visual)
1. Identify MODY subtype 2. Match to medication class 3. Initiate low-dose sulfonylurea (if applicable) 4. Reassess A1C in 3 months 5. Adjust dosage or switch to insulin if needed.
Are there any experimental or precision-medicine approaches?
Research labs are exploring CRISPR-based gene editing for rare monogenic forms, but this is still years away from clinical practice. Ongoing clinical trials are testing newer sulfonylurea derivatives that might have fewer side-effects. Keeping an eye on updates from the can help you stay informed.
How to manage the risks associated with gene-mutation diabetes?
Even though many MODY patients have a milder disease course, the usual diabetes complicationsretinopathy, nephropathy, and cardiovascular diseasestill apply if blood sugars stay high. Regular eye exams, annual kidney function tests, and a heart-healthy lifestyle are essential. Psychological support is also valuable; learning you have a genetic condition can be emotional, so counseling or support groups can make a difference.
Real-World Experience
Patient story: From misdiagnosis to a genetic cure
James, a 19-year-old college student, was diagnosed with type 1 diabetes after an emergency room visit for mild ketoacidosis. He started insulin, but his A1C hovered at 6.4% despite low insulin doses. A fellow student suggested a genetic panel. The test revealed an HNF1A mutation (MODY3). Switching to a low-dose sulfonylurea brought his A1C down to 5.6% and eliminated daily injections. James now volunteers with a local MODY awareness group, telling others, "Don't settle for the first labelask about genetics."
Clinician perspective: Why I order a MODY panel
Dr. Patel, an endocrinology fellow, shares: "When I see a patient under 25 with a family history and negative autoantibodies, I think MODY first. The panel costs around $500, but it can spare a lifetime of unnecessary insulin. Plus, it empowers families to know their risk."
Conclusion
Gene mutation diabetesa term that might sound intimidatingactually points to a highly specific and often manageable form of diabetes. By recognizing the hallmark signs, understanding how mutations differ from the broader genetics of type 1 and type 2, and considering a targeted genetic test, you can move from uncertainty to clear, personalized care.
If any of this resonated with you, or if you're curious about your own family history, I encourage you to talk to your healthcare provider about a MODY panel. A simple blood test could answer questions that have lingered for years and may even change the treatment plan for the better.
What's your experience with diabetes genetics? Have you or a loved one gone through testing? Share your story in the commentsyour insights could help someone else navigate this journey.
FAQs
What is MODY and how does it relate to gene mutations diabetes?
MODY (Maturity‑Onset Diabetes of the Young) is a form of monogenic diabetes caused by a single‑gene mutation. These gene mutations diabetes create a hereditary diabetes that is distinct from the polygenic type 1 and type 2 forms.
Which genes are most commonly linked to monogenic diabetes?
The five genes accounting for most MODY cases are GCK (MODY2), HNF1A (MODY3), HNF4A (MODY1), HNF1B (MODY5) and INS (MODY10). Each mutation produces a characteristic clinical picture.
When should I consider genetic testing for a MODY mutation?
Testing is recommended if you were diagnosed before age 25, have a strong multi‑generational family history, show negative autoantibodies, maintain a normal C‑peptide, or respond unusually well to low‑dose sulfonylureas.
What are the treatment options for the different MODY subtypes?
Most MODY2 (GCK) patients need no medication. MODY1 (HNF4A) and MODY3 (HNF1A) often respond excellently to low‑dose sulfonylureas. MODY5 (HNF1B) may require insulin, and INS‑related MODY usually needs early insulin therapy.
Can my relatives be screened for gene mutations diabetes?
Yes. Because MODY mutations have high penetrance, first‑degree relatives can be offered targeted genetic testing. Identifying carriers allows early monitoring and appropriate treatment decisions.