If you ever felt like a bite of food was getting stuck somewhere in the middle of your chest, youre probably experiencing esophageal dysphagia. Its that frustrating sensation where swallowing turns from an effortless act into a small battle. In the next few minutes, well walk through why it happens, what to watch out for, and how you can find real reliefwhether youre sitting in a doctors office or at home with a cup of tea.
Think of this as a friendly chat over coffee. Ill share the facts, sprinkle in some personal stories, and give you practical steps you can try right away. Ready? Lets dive in.
Quick-Check Summary
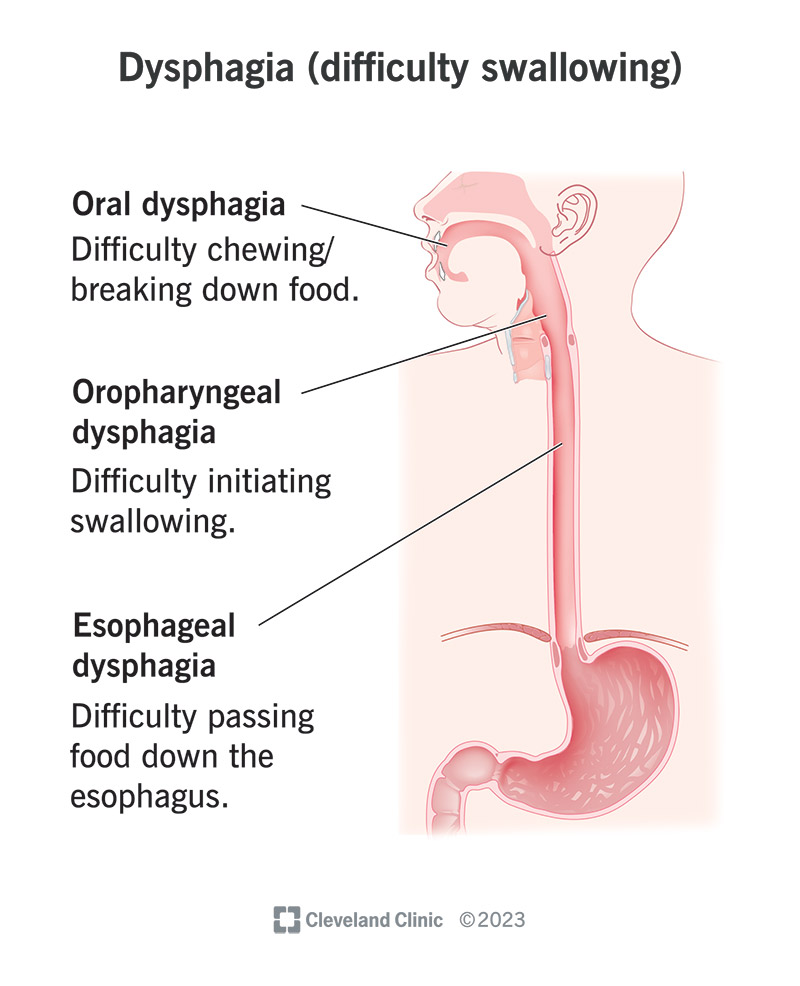
Is the problem in the esophagus or the throat?
| Feature | Esophageal Dysphagia | Oropharyngeal Dysphagia |
|---|---|---|
| Where you feel the blockage | Midchest, behind the breastbone | Back of the throat, right after the tongue |
| Typical foods that trigger | Solid foods, especially meat or bread | Any texture, often liquids also cause trouble |
| Associated pain | Retrosternal pressure or burning | Choking, coughing during meals |
What are the hallmark symptoms?
- Food sticking in the chest or feeling that it wont go down.
- Chest discomfort or a burning sensation after eating.
- Regurgitation of undigested food.
- Unexplained weight loss or loss of appetite.
- Chronic cough or hoarseness, especially after meals.
Why It Happens
Structural problems that block the esophagus
Some people develop narrow spotscalled stricturesor rings that act like tiny roadblocks. Common culprits include:
- Peptic strictures from longstanding acid reflux.
- Schatzkis ring (a thin, circumferential ring in the lower esophagus).
- Esophageal websthin membranes that can trap food.
- Tumors (benign or malignant) that grow into the lumen.
According to , early detection of strictures often prevents the need for more invasive procedures.
Motility disorders that affect movement
When the esophageal muscle doesnt contract properly, food can linger. The big players are:
- Achalasiathe lower esophageal sphincter refuses to relax.
- Diffuse esophageal spasmuncoordinated contractions that feel like a flute playing in your chest.
- Sclerodermarelated dysmotilityfibrosis stiffens the esophagus.
A 2022 review in Gastroenterology highlighted that highresolution manometry is the gold standard for diagnosing these disorders (PMCID: 6140149).
Everyday factors that can aggravate swallowing
Even lifestyle habits can tip the balance:
- Chronic GERD that inflames the esophageal lining.
- Eosinophilic esophagitisan allergic reaction causing tissue swelling.
- Medications like bisphosphonates or certain antibiotics that irritate the mucosa.
- Smoking and excessive alcohol, both of which relax the lower sphincter.
When to Worry
Is difficulty swallowing a sign of cancer?
It can be, but not always. Persistent dysphagiaespecially if you notice weight loss, pain, or blood in your salivashould prompt a prompt medical evaluation. The ICD10 code for malignant esophageal obstruction is K22.0, while benign strictures fall under K22.1. These codes help doctors quickly document and triage your condition.
Redflag symptoms that need urgent attention
- Sudden, severe difficulty swallowing.
- Unexplained weight loss >10% of body weight.
- Vomiting blood or black, tarry stools.
- Persistent odynophagia (painful swallowing).
- New onset anemia or unexplained fatigue.
If any of these pop up, head to the ER or call your healthcare provider right away.
How Doctors Diagnose
Reliable tests to pinpoint the problem
| Test | What It Shows | Pros | Cons |
|---|---|---|---|
| Barium swallow | Outline of esophageal shape, strictures, rings | Noninvasive, good for structural issues | Radiation exposure, limited motility data |
| Upper endoscopy (EGD) | Direct visualization, ability to biopsy | Gold standard for mucosal lesions | Invasive, sedation required |
| Esophageal manometry | Pressure patterns, motility disorders | Accurate for achalasia, spasm | Specialized equipment, discomfort |
| 24hour pH probe | Acid exposure, GERD severity | Helps link reflux to symptoms | Catheter discomfort, requires a few days |
Stepbystep evaluation flow
- Detailed medical history (when symptoms started, foods that trigger).
- Physical exam focusing on neck, chest, and neurologic signs.
- Initial imagingusually a barium swallow.
- If structural abnormality is suspected, proceed to upper endoscopy.
- When motility is a concern, schedule highresolution manometry.
- Discuss findings with a gastroenterologist and plan treatment.
Treatment Options
Medical pathways doctors typically follow
Depending on the cause, treatment can range from a simple prescription to a minimally invasive procedure.
- Pharmacologic therapy: Protonpump inhibitors for refluxrelated strictures; calcium channel blockers or nitrates for esophageal spasm.
- Endoscopic dilation: Balloon or bougienage to gently stretch a narrowed segment.
- Stent placement: Temporary metal or plastic tubes keep the lumen open, often used for malignant obstruction.
- Peroral endoscopic myotomy (POEM): A modern, scarfree technique for achalasia.
- Surgical options: Heller myotomy or tumor resection when endoscopy isnt enough.
Can I manage symptoms at home?
Absolutelymany folks find relief with a few practical tweaks while they await medical care.
- Diet modifications: Stick to soft foods (mashed potatoes, yogurt) and cut everything into bitesize pieces. Chew thoroughlythink of each bite as a tiny rehearsal.
- Swallowing techniques: The chintuck (tuck your chin toward your chest while swallowing) can help shorten the distance food travels.
- Overthecounter aids: Antacids or alginate formulations reduce acid irritation that may exacerbate strictures.
- Lifestyle changes: Elevate the head of your bed 68 inches, avoid latenight meals, and limit caffeine/alcohol.
These often bridge the gap until you see a specialist.
When speechlanguage pathology helps
Swallowing therapists guide you through the 4 stages of dysphagiascreening, intervention, maintenance, and discharge. They teach exercises that strengthen the upper esophageal sphincter and improve coordination, turning a daunting task into a series of manageable steps.
Living With Esophageal Dysphagia
Keeping nutrition on track
Malnutrition is a real risk, but a wellplanned menu can keep you fueled.
- Highprotein smoothies (Greek yogurt, nut butter, banana) blended smooth enough to glide down.
- Fortified soupsadd powdered whey or maltodextrin for extra calories.
- Small, frequent meals instead of three big ones; think snackstyle eating.
Emotional side of swallowing trouble
I once chatted with a patient named Javier who described mealtime as a daily anxiety test. He felt isolated because friends would order steaks while he could only manage soft pasta. After a few sessions with a speech therapist and a slight diet overhaul, Javier regained confidenceand even started a supportive online group for others with dysphagia. Stories like his remind us that the psychological impact can be just as heavy as the physical blockage.
Trusted resources you can count on
- Patient support groups on platforms like Reddits r/SwallowingDisorders.
These sites are a great starting point for credible, uptodate information.
Bottom Line Take Action Today
Key takeaways
- Esophageal dysphagia feels like food sticking in the chest and can stem from structural blocks or motility issues.
- Redflag signsweight loss, pain, bloodrequire prompt medical attention.
- Diagnosis typically involves a barium swallow, endoscopy, and sometimes manometry.
- Treatment ranges from medication and diet changes to endoscopic dilation or surgery.
- Home strategiessoft diet, chintuck, lifestyle tweakscan ease symptoms while youre in care.
Your next steps
If youve noticed any of the symptoms above, reach out to your primary care provider or a gastroenterologist. Ask about a barium swallow or an upper endoscopy to get a clear picture of whats happening inside.
Meanwhile, try swapping a tough piece of steak for a creamy mushroom risotto and practice the chintuck technique at home. Small adjustments can make a big difference while you await professional guidance.
Feel free to share your experience in the commentswhats worked for you, whats still a mystery? Were all in this together, and your story might be the reassurance someone else needs.
Conclusion
Living with esophageal dysphagia can feel like navigating a maze where the exit isnt always clear. By understanding the common causes, recognizing warning signs, and taking both medical and athome steps, you can turn confusion into control. Remember, you dont have to face this alonedoctors, speech therapists, and a supportive community are ready to help you reclaim the simple joy of a carefree bite.
For people who also manage related gut issues, learning about gentle approaches like gastroenteritis home remedies can be useful when temporary upset stomach or vomiting worsens swallowing symptoms.
FAQs
What is esophageal dysphagia?
Esophageal dysphagia is the sensation that food is sticking or getting caught in the chest or lower throat after swallowing, often caused by structural or motility problems in the esophagus.
What are the common causes of esophageal dysphagia?
Common causes include esophageal strictures from acid reflux, Schatzki’s ring, tumors, esophageal webs, achalasia, esophageal spasms, GERD, eosinophilic esophagitis, and scleroderma-related motility disorders.
When should I see a doctor for esophageal dysphagia?
You should seek urgent medical care if you experience sudden severe swallowing difficulty, unexplained weight loss, vomiting blood, persistent painful swallowing, or anemia.
How is esophageal dysphagia diagnosed?
Diagnosis often involves a barium swallow X-ray, upper endoscopy to visualize the esophagus, esophageal manometry for motility assessment, and sometimes a 24-hour pH probe to check for acid reflux.
Can esophageal dysphagia be treated at home?
Symptom relief at home includes eating soft, bite-sized foods, practicing swallowing techniques like the chin-tuck, using antacids for acid irritation, and lifestyle changes such as elevating the head of the bed and avoiding late meals.