If youve just learned that cirrhosis has knocked your platelet count down, youre probably asking two things: Can I raise it? and What will happen if I dont? The short answer is yes there are several ways to boost platelets, each with its own pros and cons. This article walks you through why platelets fall in liver disease, when doctors decide to intervene, and which treatments (from transfusions to tasty lifestyle tweaks) might be right for you.
Grab a cup of tea, settle in, and lets untangle the world of thrombocytopenia in cirrhosis treatment together. Ill share the science, the stories, and a few practical tips you can start using today.
Why Platelets Drop
What is thrombocytopenia and whats normal in cirrhosis?
Thrombocytopenia simply means low platelet count. In a healthy adult, platelets usually hover between 15040010/L. In cirrhosis, especially when the disease is advanced, counts often slide below 10010/L, and in decompensated cirrhosis they can dip even further.
Why does cirrhosis cause low platelets?
The liver does more than filter toxins; it also makes thrombopoietin, the hormone that tells your bone marrow to crank out platelets. When scar tissue builds up, the livers ability to produce this hormone drops. Add a swollen spleen (splenomegaly) which grabs and holds onto platelets and youve got a perfect storm. Portal hypertension, the high blood pressure in the vein that feeds the liver, pushes blood into the spleen, making it even larger and more grabby.
Endstage liver disease low platelet count vs. earlier stages
| Stage | Typical Platelet Range | Key Drivers |
|---|---|---|
| Compensated cirrhosis | 10015010/L | Mild thrombopoietin drop, early splenic sequestration |
| Decompensated cirrhosis | 5010010/L | Significant portal hypertension, larger spleen |
| Endstage/acute decompensation | <5010/L | Severe thrombopoietin deficiency, massive splenomegaly, bonemarrow suppression |
When to Treat
Key labs and imaging youll see
Besides the routine CBC, doctors usually order an abdominal ultrasound to check spleen size and a FibroScan or elastography to gauge liver stiffness. These images help decide whether the low platelet count is just a lab number or a red flag for bleeding risk.
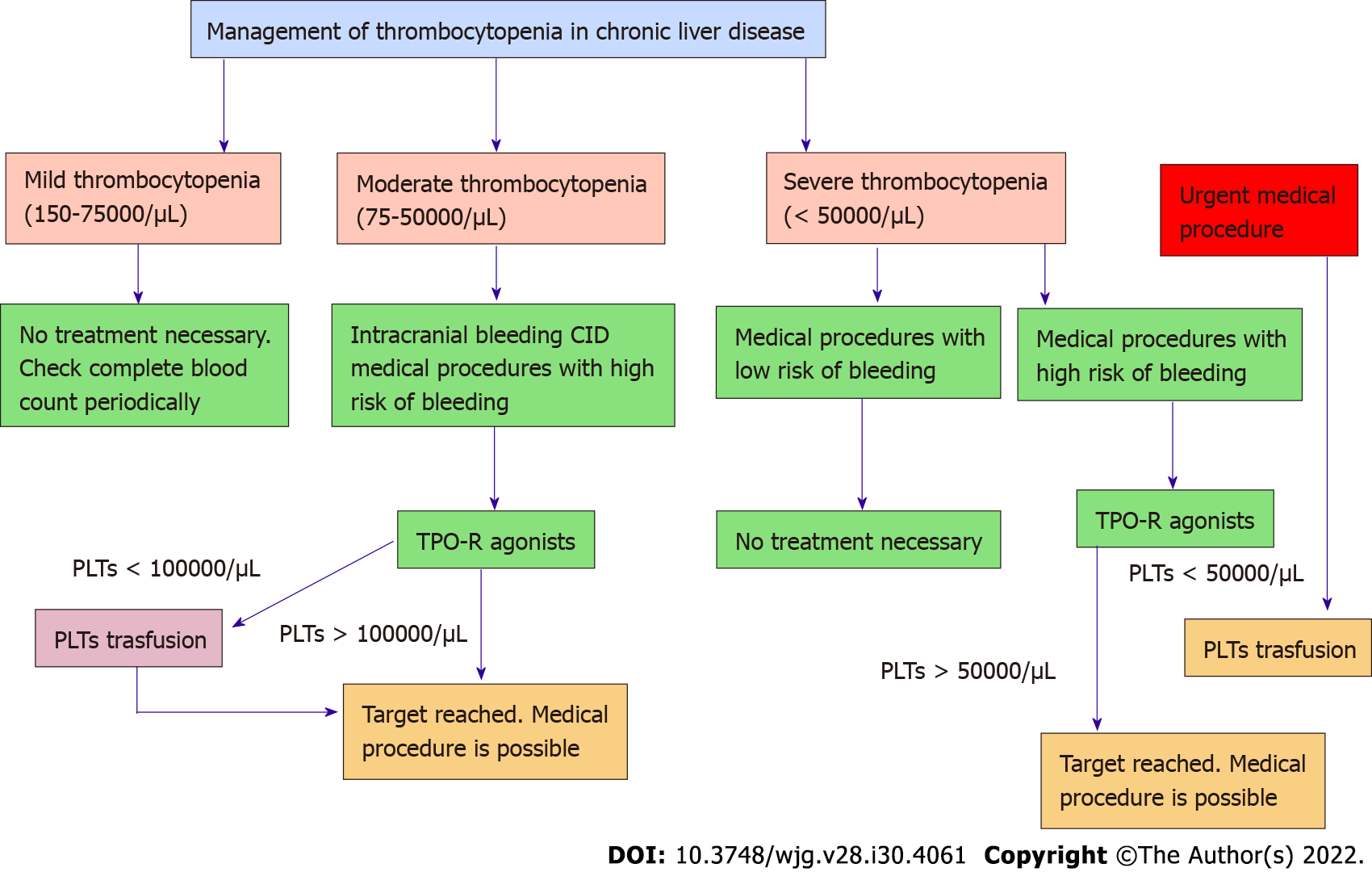
Thresholds for action
Most hepatology societies recommend intervening when platelets fall below 5010/L before an invasive procedure (like a liver biopsy or endoscopy). If youre heading into major surgery, the safety line is often 3010/L. Below that, the risk of spontaneous bleeding spikes dramatically.
Redflag situations
- Active variceal bleeding you need a rapid rise, usually via transfusion.
- Pretransplant workup transplant teams prefer counts >7510/L.
- Upcoming elective surgeries even a minor orthopedic repair can become risky.
Treatment Options
Platelet transfusion the instant fix
When time is of the essence, a platelet transfusion can raise the count by 203010/L within minutes. Its the goto for emergency bleeds or before a highrisk endoscopic banding. The downside? The effect lasts only a few days, and theres a small chance of allergic reactions or infections.
Thrombopoietinreceptor agonists (TPORAs)
Oral medications like avatrombopag and lusutrombopag stimulate your bone marrow to make more platelets. Theyre especially handy when you have a scheduled procedure a week or two away. Studies show they can lift counts into the safe range without the need for a transfusion.
According to a , avatrombopag achieved platelet counts 5010/L in 85% of patients, with a low incidence of thrombotic events.
Partial splenic embolization (PSE)
This radiologic technique blocks part of the splenic artery, shrinking the organs ability to hoard platelets. It offers a sustained rise (often staying >8010/L for months) while avoiding a fullblown surgery. You may feel some postprocedure pain, but most people recover in a week.
Surgical splenectomy open vs. laparoscopic
Removing the spleen outright eliminates the biggest platelet sink. Modern laparoscopic splenectomy, first reported in the early 1990s, brings the benefits of smaller incisions, less pain, and quicker discharge compared with the traditional open approach.
A review of 1,200 patients showed laparoscopic splenectomy reduced hospital stay from 7days (open) to 3days, with comparable longterm platelet improvements.
When to choose what?
| Option | How It Works | Best For | Major Risks |
|---|---|---|---|
| Platelet transfusion | Direct infusion of donor platelets | Acute bleeding, immediate preprocedure | Allergic reaction, shortduration effect |
| TPORA (avatrombopag, lusutrombopag) | Stimulates bonemarrow platelet production | Elective procedures, chronic low counts | Potential thrombosis, cost |
| Partial splenic embolization | Radiologic reduction of splenic function | Moderatesevere thrombocytopenia, poor surgical candidate | Pain, fever, rare splenic abscess |
| Laparoscopic splenectomy | Removal of the spleen | Severe, refractory thrombocytopenia, large spleen | Postsplenectomy infection, operative mortality |
Natural Boosts & Lifestyle Tweaks
Nutrition that helps
While food alone wont fix splenic sequestration, certain nutrients give your marrow a friendly nudge. Think leafy greens for folate, lean meats for iron, and dairy or fortified cereals for vitaminB12. VitaminK (found in broccoli, kale, and Brussels sprouts) supports platelet function, though it doesnt raise the count.
Lifestyle habits
- Avoid alcohol. Even a small amount can suppress bonemarrow production.
- Quit smoking. Nicotine interferes with platelet aggregation.
- Stay active. Light exercise improves circulation and can mildly boost platelet turnover.
- Manage infections promptly. Fever spikes can temporarily worsen thrombocytopenia.
Complementary approaches
Some patients report modest improvements with herbal formulas that contain milk thistle or dandelion, but the evidence is anecdotal at best. If you experiment, keep your hepatologist in the loop we dont want hidden interactions.
When natural isnt enough
If youve tried diet and lifestyle changes for a few weeks and your count remains under 7010/L, its time to discuss medical options. Ignoring a persistently low count can increase bleeding risk, especially if you develop varices or need a liver transplant. For patients who also struggle with symptoms like constipation related to pelvic floor dysfunction, consider discussing targeted treatments such as pelvic floor constipation evaluation with your care team addressing concurrent issues can improve overall recovery and quality of life.
DecisionMaking Framework
Step1: Assess severity
Take note of three numbers: platelet count, spleen size on ultrasound, and liver function scores (ChildPugh or MELD). A patient with 4510/L, a spleen 16cm wide, and MELD=16 is a different case from someone with 9010/L, a modest spleen, and MELD=8.
Step2: Identify goals
Are you planning a liver transplant? Are you about to undergo an endoscopic variceal ligation? Or are you simply trying to feel safer in daily life?
Step3: Match options
Heres a quick flowchart you can sketch on a napkin:
- If platelets<3010/L consider immediate platelet transfusion.
- If 305010/L + splenomegaly discuss partial splenic embolization or laparoscopic splenectomy.
- If 508010/L + elective procedure in 24weeks try a TPORA.
- If >8010/L and stable focus on nutrition and lifestyle.
Step4: Shared decision
Bring these points to your hepatology team. Ask them about success rates, costs, and recovery time. A good doctor will respect your preferences and help you weigh the benefits against the risks.
Common Questions (Quick Answers)
Why does cirrhosis cause low platelets?
Because scarred liver tissue makes less thrombopoietin and portal hypertension enlarges the spleen, which traps platelets.
Can I raise my platelets without medication?
Diet, exercise, and avoiding alcohol can help modestly, but most people need medical therapy when counts drop below 7010/L.
Is splenectomy safe in decompensated cirrhosis?
When performed laparoscopically by an experienced team, its generally safe, though the risk of infection is higher than in healthy patients.
Whats the difference between avatrombopag and lusutrombopag?
Both are TPOreceptor agonists; avatrombopag is taken once daily for 5 days before a procedure, while lusutrombopag is usually a 7day course. Their efficacy is comparable, but dosing schedules differ.
How long does a platelet transfusion last?
Usually 25 days, after which the count returns to baseline unless another intervention is added.
Sources & Further Reading
For deeper dives, you can check the American Association for the Study of Liver Diseases (AASLD) 2024 guidelines, the recent review in Hepatology on splenic interventions, and a metaanalysis on TPOreceptor agonists published in MDPI. All data cited are uptodate as of August2025.
Conclusion
Living with cirrhosis and a low platelet count can feel like walking a tightrope, but youre not alone. The livers failure to produce thrombopoietin and an overactive spleen are the main culprits behind thrombocytopenia. Fortunately, you have options ranging from rapidacting transfusions to oral drugs that let your body do the heavy lifting, plus interventional radiology or surgical routes for longerterm relief. Pair those medical tools with sensible nutrition, a boozefree lifestyle, and regular checkins with your hepatology team, and youll give yourself the best chance of staying safe and feeling well.
Whats your experience with low platelets and cirrhosis? Have you tried a TPOagonist or found a particular diet helpful? Share your story with a trusted friend or health professional the more we talk, the more we learn.
FAQs
Why does cirrhosis cause low platelets?
Cirrhosis reduces thrombopoietin production and enlarges the spleen, which traps platelets, leading to thrombocytopenia.
Can I raise my platelets without medication?
Diet, exercise, and avoiding alcohol may help modestly, but most people need medical therapy when platelets drop below 70×10⁹/L.
Is splenectomy safe in decompensated cirrhosis?
Laparoscopic splenectomy is generally safe in decompensated cirrhosis when performed by experienced teams, though infection risk is higher.
What’s the difference between avatrombopag and lusutrombopag?
Both are TPO receptor agonists; avatrombopag is a 5-day course, lusutrombopag is usually a 7-day course, with similar efficacy.
How long does a platelet transfusion last?
A platelet transfusion typically raises counts for 2–5 days before levels return to baseline.