If youre scrolling through endless pages looking for a clear answer, heres the short version: the most effective endometriosis treatment blends painrelief medication, hormonal therapy, and, when needed, surgery. Below youll find a practical guide that explains each option, its benefits, and its risks so you can decide what feels right for you.
Every womans journey with endometriosis is unique. Whether youre managing mild symptoms or coping with stage4 disease, the choices you make now can shape both your comfort today and your plans for the future (like fertility or quality of life). Lets walk through the basics, the core treatments, and how to create a plan that matches your goals.
Understanding the Basics
What Causes Endometriosis?
Scientists still piece together the puzzle, but the leading theories point to hormonal imbalances, retrograde menstruation (where menstrual blood flows backward into the pelvic cavity), genetic predisposition, and inflammation. According to , a combination of these factors likely triggers the tissue that normally lines the uterus to grow outside it.
How Is Endometriosis Diagnosed?
Diagnosis often starts with a detailed symptom diary and a pelvic exam. Imaging tools like ultrasound or MRI can spot larger lesions, but the gold standard remains laparoscopy a minimally invasive surgery that lets doctors see and remove tissue while confirming the diagnosis.
Stages of Endometriosis (14)
| Stage | Extent of Tissue | Typical Treatment Approach |
|---|---|---|
| Stage1 (Minimal) | Few superficial implants | Hormonal therapy, NSAIDs |
| Stage2 (Mild) | More implants, some deeper lesions | Combination hormonal therapy + pain management |
| Stage3 (Moderate) | Multiple deep lesions, possible ovarian cysts | Hormonal therapy laparoscopic excision |
| Stage4 (Severe) | Extensive implants, severe adhesions, large cysts | Often surgery + longterm hormonal suppression |
20 Common Symptoms of Endometriosis
Because every body is different, you might experience just a handfulor manyof the following signs. If you recognize several, its worth talking to a specialist:
- Painful periods (dysmenorrhea)
- Heavy menstrual bleeding
- Pelvic pain during or after intercourse (dyspareunia)
- Chronic lowerback or abdominal pain
- Painful bowel movements or urination during periods
- Fatigue and low energy
- Infertility or difficulty getting pregnant
- Irregular cycles
- Spotting between periods
- Enlarged ovaries or ovarian cysts (endometriomas)
- Digestive issues (bloating, constipation)
- Unexplained weight changes
- Menstrual cramps that just wont quit
- Feeling of pressure in the pelvis
- Leg pain or numbness (if nerves are involved)
- Hair loss or thinning (rare hormonal effect)
- Joint pain or muscle aches
- Hot flashes unrelated to menopause
- Emotional mood swings
- Reduced sexual desire
Core Treatment Options
Hormonal & Medication Therapies
Combined Oral Contraceptives (COC) The pills keep ovulation on pause, which reduces the hormonal stimulus that fuels endometrial growth. Many women love the added benefit of lighter periods, though some may experience breakthrough spotting.
Progestins & ProgestinOnly IUDs These deliver a steady dose of hormone directly to the uterus, thinning the lining and often shrinking implants. The levonorgestrel IUD is a favourite for those who want longterm relief without daily pills.
GnRH Agonists/Antagonists By essentially turning off the ovaries, these drugs create a temporary menopauselike state. Theyre powerful for severe cases, especially before surgery, but are usually limited to six months because of bonedensity concerns. Adding addback estrogen or progesterone helps mitigate those side effects.
NSAIDs & Pain Relievers Overthecounter options like ibuprofen can blunt the inflammatory component of pain. Theyre best for mildtomoderate flareups, but they wont address the underlying tissue growth.
Emerging Therapies Researchers are exploring aromatase inhibitors and selective progesterone receptor modulators (SPRMs) as alternatives, especially for women who cant tolerate traditional hormones. A recent highlighted promising symptom reduction, though longterm data are still pending.
Surgical Options
Laparoscopic Excision & Ablation This minimally invasive approach lets surgeons cut out or destroy lesions while preserving healthy tissue. For stage34 disease, laparoscopy is often the goldstandard because it offers both diagnosis and treatment in one go.
RoboticAssisted Laparoscopy The robot provides enhanced precision, which can be beneficial when lesions are tucked near delicate structures like the ureters. Its typically reserved for complex cases and may not be covered by all insurers.
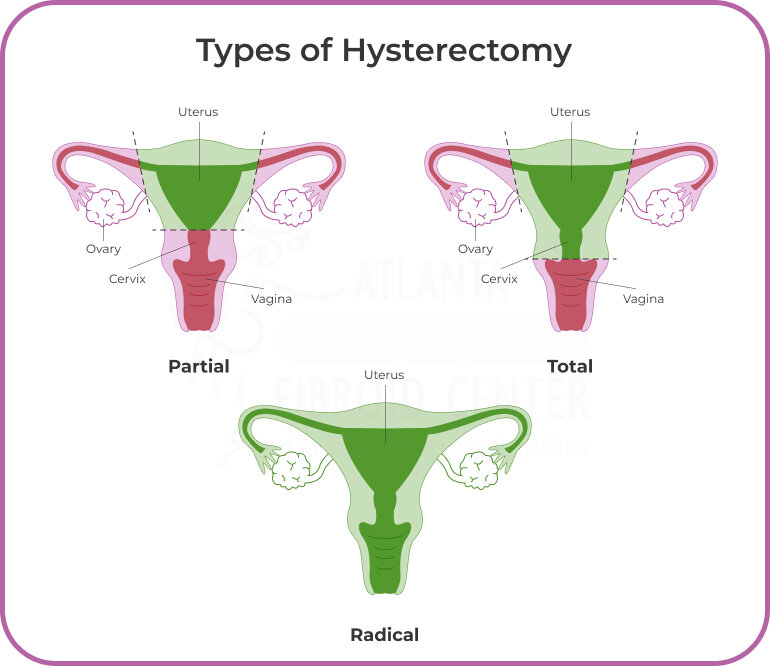
Hysterectomy & Oophorectomy In rare, refractory casesespecially when a woman has completed childbearingremoving the uterus (hysterectomy) and/or ovaries (oophorectomy) can eradicate disease. This is a lastresort option because it ends fertility and induces menopause, requiring hormone replacement therapy.
PostSurgery Hormonal Maintenance Even after a successful excision, most surgeons recommend continuing hormonal suppression for several months to prevent recurrence. Think of it as maintenance therapy that protects the hardwon results of surgery.
Choosing Your Plan
Pain Management vs. Fertility Goals
Ask yourself: Is my primary goal to get rid of pain now, or to preserve my chances of getting pregnant later? If fertility is a priority, many doctors start with hormonal suppression that can be paused for a timed conception cycle, or they may opt for targeted laparoscopic removal of lesions that threaten the ovaries. If you are exploring how endometriosis affects childbearing specifically, read more about lean PCOS fertility as some overlapping fertility considerations and treatments can apply in multidisciplinary care plans.
StageSpecific Recommendations
For stage12, most women find relief with hormonal therapy (COC or progestin IUD) plus NSAIDs. Stage3 often calls for a mixstart with medication, assess response, then consider surgery if pain persists. Stage4 usually requires surgery followed by longterm hormonal suppression; the good news is that, according to the , many women achieve significant symptom improvement after combined treatment.
Balancing Risks & Benefits
| Treatment | Benefits | Common Risks | Recovery Time |
|---|---|---|---|
| COC | Reduced pain, lighter periods | Spotting, mood changes, rare clotting | Immediate (no downtime) |
| Progestin IUD | Longterm relief (35years) | Irregular bleeding, device expulsion | Sameday insert, brief soreness |
| GnRH Agonist | Powerful symptom suppression | Hot flashes, bone loss, mood swings | 6month course, addback therapy needed |
| Laparoscopic Excision | Direct removal, fertilitypreserving | Bleeding, infection, adhesion formation | 12weeks off work, full recovery 46weeks |
Lifestyle & Complementary Support
Medication and surgery are powerful, but lifestyle tweaks can boost results. Regular exerciseespecially lowimpact activities like swimming or yogahelps reduce inflammation. A diet rich in omega3 fatty acids (fish, flaxseed) and low in processed sugars may also ease symptoms. Stress management techniquesmindfulness, breathing exercises, or even a supportive therapistcan lower pain perception, as chronic stress feeds hormonal imbalances.
When to Seek a Second Opinion
If youve tried a treatment for several months without meaningful relief, or if you feel your doctor isnt addressing fertility concerns, its perfectly okay to get another perspective. Look for a specialist who regularly publishes research or is affiliated with a reputable center (e.g., Mayo Clinic, Cleveland Clinic, Johns Hopkins). A fresh review can uncover missed lesions or suggest alternative therapies.
Helpful Resources & Next Steps
Below are a few trusted resources you might find useful:
- patient stories, research updates, and a directory of specialist centers.
- comprehensive overview of causes, diagnosis, and treatment guidelines.
- clear explanations of medication options and surgical procedures.
How to Prepare for Your First Appointment
- Write down a monthlong symptom diary (pain levels, cycle dates, bowel habits).
- List your top priorities (pain relief, fertility, hormonefree options).
- Bring any previous imaging reports or surgical notes.
- Prepare questions: Whats the success rate of laparoscopy for stage3 disease? or How will this medication affect my bone health?
If youre ready to take the next step, consider downloading a . It walks you through the pros and cons of each option and helps you articulate your preferences to your doctor.
Conclusion
Endometriosis treatment isnt a onesizefitsall road map. The best plan blends scientific evidence, professional expertise, and your personal goalswhether thats pain relief, fertility, or preserving hormone balance. By understanding the causes, recognizing the full spectrum of symptoms, and weighing the benefits against the risks, you can make an informed decision that feels right for you.
Remember, you dont have to navigate this alone. Trusted medical centers, supportive communities, and reliable online resources are just a click away. Share your thoughts or experiences in the commentsyour story might be the beacon someone else needs. If you have questions, feel free to ask; were all in this together.
FAQs
What are the main treatment options for endometriosis?
The main treatments include pain-relief medications like NSAIDs, hormonal therapies such as combined oral contraceptives and progestin IUDs, and surgical options including laparoscopic excision and, in severe cases, hysterectomy.
How does hormonal therapy help endometriosis?
Hormonal therapies work by reducing or stopping ovulation and thinning the uterine lining, which helps shrink endometrial implants and relieve pain. Examples are birth control pills, progestins, and GnRH agonists.
When is surgery recommended for endometriosis?
Surgery is advised for moderate to severe stages (stage 3 and 4), especially when pain persists despite medication or when fertility preservation is a goal. Laparoscopy is the preferred minimally invasive surgery.
Can endometriosis treatment affect fertility?
Yes, treatment plans often consider fertility goals. Hormonal therapies can be paused for conception attempts, and surgical removal of lesions near ovaries can improve fertility chances.
Are there risks associated with endometriosis treatments?
Each treatment has risks: hormonal therapies may cause spotting or mood changes, GnRH agonists can lead to bone loss, and surgery carries risks of bleeding, infection, and adhesions.