Key Differences Overview
First, lets lay the ground rules. Reactive arthritis is a postinfectious, immunemediated reaction that usually follows a gastrointestinal or genitourinary infection. Think afterthestorm inflammation that brings eyes, skin, or urinary symptoms into the mix. Septic arthritis, on the other hand, is a fullblown bacterial infection inside the joint itself an emergency that can wreck cartilage in hours if you dont act fast.
Why does this matter for the USMLE? Because the exam loves to test your ability to differentiate based on history, jointfluid analysis, and urgency of treatment. Nail those three pillars, and youll ace the question faster than you can finish a coffee break.
Clinical Presentation Clues
Imagine two patients walking into the ER. One is a 22yearold college student who just recovered from dysentery; he now has a swollen knee, a pink eye, and a burning urination. The other is a 45yearold carpenter with a high fever, chills, and a single, hugely swollen knee that looks like a balloon.
| Feature | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Onset | 14weeks after GI/GU infection | Within 48hours of systemic symptoms |
| Joint Involvement | Often asymmetric, lowerextremity, oligoarticular | Usually monoarticular, most often knee |
| Systemic Signs | Lowgrade fever, conjunctivitis, urethritis, skin lesions (reactive arthritis triad) | High fever, rigors, severe pain |
| Joint Fluid | Sterile, WBC 2005000 (neutrophilpredominant) | Purulent, WBC>50000, positive culture |
| Lab Markers | Elevated ESR/CRP, frequently HLAB27 positive | Marked leukocytosis, positive blood cultures |
Notice the triad of arthritis, conjunctivitis, and urethritis? Thats the youll see on the exam. Septic arthritis doesnt care about eye redness; it cares about rapid joint destruction.
Diagnostic Workup Steps
When the USMLE asks whats the next best step? picture yourself in the ER with a joint tap kit in hand.
- Joint aspiration: Draw synovial fluid, send for Gram stain, culture, and cell count. A sterile fluid leans toward reactive arthritis; a purulent smear screams septic.
- Blood work: CBC, ESR, CRP, and blood cultures. Dont forget HLAB27 testing when you suspect reactive arthritis (about 70% of patients are positive).
- Imaging: Plain Xray first (to rule out osteomyelitis), then ultrasound or MRI if you need to see effusion or early bone changes.
One clinical anecdote Ill never forget: during my third-year rotation, a patients fever spiked just as I was about to send the fluid for culture. My attending ordered an immediate arthrocentesis, and the Gram stain showed Grampositive cocci in clusters classic MSSA septic arthritis. That quick decision saved the joint and the patients exam grade.
Treatment Strategies Overview
Now, the dreaded treatment part. The strategies diverge dramatically.
Reactive Arthritis Treatment
First, treat the underlying infection (if its still active) with a short course of antibiotics usually azithromycin for Chlamydia or a fluoroquinolone for enteric bugs. Then, manage joint inflammation:
- NSAIDs are firstline (ibuprofen, naproxen).
- If pain persists, consider a short taper of oral steroids.
- Refractory cases may need DMARDs like sulfasalazine or even a TNF inhibitor (especially if the patient is HLAB27 positive).
According to , most patients see symptom resolution within 612 months, but a minority develop chronic arthritis.
Septic Arthritis Treatment
Time is cartilage. The mantra is drain and antibiotics, ASAP.
- Empiric IV antibiotics: Nafcillin or cefazolin for MSSA; vancomycin if MRSA is a concern. Adjust based on culture results.
- Joint drainage: Needle aspiration (often repeated), arthroscopy, or open surgical drainage depending on joint and organism.
- Hospitalization: Admit all patients for monitoring, serial labs, and repeat imaging.
A study in the New England Journal of Medicine highlighted that delayed drainage beyond 12hours doubles the risk of permanent joint damage, underscoring why the USMLE loves this scenario.
HighYield Comparison Tables
When you stare at a wall of text during a practice test, a quick table can be a lifesaver. Below is a cheatsheet you can memorize or paste into your flashcards.
| Aspect | Reactive Arthritis | Septic Arthritis | Rheumatoid Arthritis | Osteomyelitis |
|---|---|---|---|---|
| Typical Trigger | GI/GU infection | Bacterial invasion | Autoimmune | Bone infection |
| Joint Fluid | Sterile, 2005000 WBC | Purulent, >50000 WBC | Elevated RF, ACPA | Often negative |
| Systemic Fever | Lowgrade | High, spikes | Lowmoderate | Variable |
| Key Extraarticular | Conjunctivitis, urethritis | None typical | Rheumatoid nodules | Localized bone pain |
Memorize the RSRO pattern (Reactive, Septic, Rheumatoid, Osteomyelitis) and youll have a mental scaffold for any related board question, including those that mix in reactive arthritis vs rheumatoid arthritis or septic arthritis vs osteomyelitis.
Related Quick FAQs
Here are a few bitesize answers that often pop up in practice questions.
- Reactive arthritis vs postinfectious arthritis: Theyre essentially the same; postinfectious is a broader term that includes reactive arthritis as a subset.
- Transient synovitis vs reactive arthritis: Transient synovitis is a benign, selflimited hip inflammation in kids, usually without systemic signs or a preceding infection.
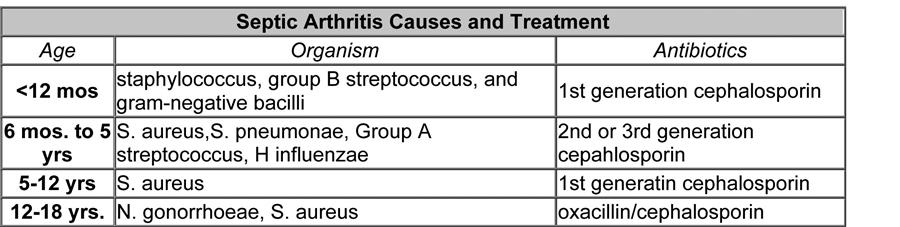
- Causes of septic arthritis: Staphylococcus aureus is the leader, followed by Streptococcus species, Neisseria gonorrhoeae (in sexually active teens), and gramnegative rods in immunocompromised patients.
- Reactive arthritis treatment: NSAIDs steroids (if needed) DMARDs for chronic cases.
USMLE Day Tips
When the exam clock starts ticking, a quick mental checklist can keep you from panicking.
- History first: Recent diarrhea, dysentery, or urethritis? Think reactive. If the history mentions prolonged back pain with morning stiffness improving with exercise, also consider looking up criteria for ankylosing spondylitis to avoid misclassification see ankylosing spondylitis criteria for quick differentiation tips.
- Joint fluid count: Under 5,000 = reactive; Over 50,000 = septic.
- Red flags: Fever > 38.5C, severe pain, inability to bear weight septic, treat now.
- Mnemonic: RSAT Reactive (postinfection), Septic (infection), Antibiotics (IV), Treatment (drain).
And remember, the USMLE loves you to be systematic. If you can verbally walk through the algorithmHistory Fluid Imaging Managementyoull score points for clinical reasoning, not just memorization.
Conclusion
Summing it all up: reactive arthritis is an immunemediated aftermath of a GI or GU infection, marked by the triad of arthritis, conjunctivitis, and urethritis, while septic arthritis is an urgent bacterial invasion of the joint that demands immediate drainage and IV antibiotics. By focusing on the timeline of symptoms, the nature of joint fluid, and the presence (or absence) of systemic signs, you can confidently differentiate these two conditions on the USMLE and, more importantly, on the wards.
Got a study tip that helped you conquer a tough arthritis question? Share it in the comments below. If youre still unsure about any of the steps, feel free to asklets ace this together!
FAQs
What are the main clinical differences between reactive arthritis and septic arthritis on the USMLE?
Reactive arthritis follows a GI/GU infection, is often asymmetric, presents with conjunctivitis/urethritis, and has low‑grade fever. Septic arthritis appears abruptly with high fever, severe mono‑articular pain, and rapid joint destruction.
How is joint fluid analysis used to distinguish reactive from septic arthritis?
Reactive arthritis yields sterile fluid with WBC 200‑5 000 (neutrophil‑predominant). Septic arthritis shows purulent fluid with WBC > 50 000 and a positive Gram stain/culture.
What is the first‑line treatment for reactive arthritis in a USMLE question?
Begin NSAIDs for pain control; add a short course of antibiotics if the triggering infection is active, and consider steroids or DMARDs for refractory disease.
Which organisms most commonly cause septic arthritis that appears on the USMLE?
Staphylococcus aureus is the top cause, followed by Streptococcus species, Neisseria gonorrhoeae in sexually active teens, and gram‑negative rods in immunocompromised patients.
When should you prioritize urgent joint drainage for suspected septic arthritis?
Any patient with high fever, severe joint pain, inability to bear weight, or synovial fluid WBC > 50 000 requires immediate arthrocentesis and drainage within 12 hours.