If youve ever Googled decorticate posturing survival rate, you were probably looking for a straight answer and you deserve one, right now. Roughly 37% of people who develop decorticate posturing after a brain injury survive longterm. The rest either succumb to the injury or live with severe disability.
That figure isnt the whole story, though. Survival chances swing dramatically when you compare decorticate with decerebrate posturing, when you consider how quickly care is delivered, and when you look at where the brain damage actually sits. Lets unpack those numbers together, without the medical jargon clouding the view.
Quick Summary Stats
Overall Survival Percentages
Across multiple neurology studies, the average survival rate for decorticate posturing hovers around 3540%. By comparison, decerebrate posturing a sign of deeper brainstem injury drops to about 10%. Those numbers are sobering, but they also give families a concrete starting point for discussion with doctors.
Mortality Range in Literature
Research from institutions like the reports mortality rates of 6883% for patients showing decerebrate posturing, especially when pupils are fixed and dilated. Decorticate posturings mortality is lower, but still significant often 6070% when compounded by other poor prognostic signs.
Outcome Comparison Table
| Aspect | Decorticate Posturing | Decerebrate Posturing |
|---|---|---|
| Typical Survival Rate | 37% | 10% |
| Common Causes | Severe TBI, intracranial bleed, seizures | Brainstem compression, massive hemorrhage |
| Brain Areas Affected | Damage above red nucleus (corticospinal tract) | Damage at/ below the midbrain |
| Prognostic Indicators | Reactive pupils = better odds | Fixed, dilated pupils = poor odds |
What Is Decorticate
Definition and Appearance
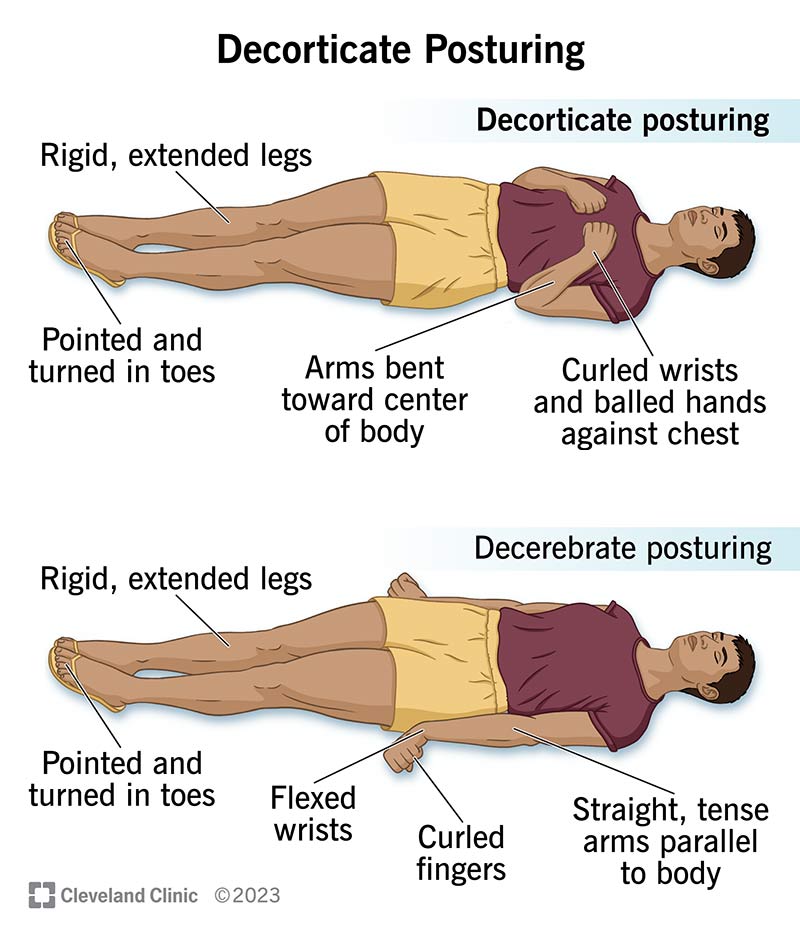
Decorticate posturing is that classic arms flexed, legs extended posture you might see in medical dramas. The shoulders are rounded forward, elbows are bent, wrists flex, and the legs straighten as if the person is trying to brace themselves against an invisible force. This tells us the injury is somewhere above the red nucleus in the brain think of it as a signal from the upper motor pathways that somethings very wrong up top.
Common Triggers
Things that can tip the brain into this posture include:
- Severe traumatic brain injury (a car crash, a fall from a height)
- Large intracerebral hemorrhage or subdural hematoma
- Ischemic stroke affecting the middle cerebral artery territory
- Seizure activity that spikes intracranial pressure yes, a decorticate posturing seizure can look like a prolonged convulsion followed by the classic flexed posture.
Which Part of the Brain Is Hurt?
The phrase decorticate posturing damage to what part of brain usually points to the corticospinal tractthe highway that carries voluntary movement signals from the motor cortex down through the internal capsule and into the spinal cord. When that tract gets interrupted above the red nucleus (located in the midbrain), the brain cant properly coordinate the extensor muscles in the arms, so they default to flexion.
Decerebrate vs Decorticate
Which Is Worse?
The short answer: decerebrate posturing is generally worse. Decerebrate posture shows that the injury has slipped down to the brainstem, a region that controls vital functions like breathing and heart rate. Thats why the survival rate drops to roughly ten percent.
What Does Decerebrate Indicate?
When a patients arms and legs are both extended with the wrists flexed, the brain is basically shouting everything below the midbrain is out of sync. This pattern often indicates severe brainstem compression, massive hemorrhage, or a catastrophic increase in intracranial pressure.
Why Is Decerebrate Worse?
Two main reasons:
- Loss of protective reflexes: The brainstem houses the gag and cough reflexes. When its damaged, the patient cant protect their airway, leading to aspiration and pneumonia.
- Autonomic instability: Blood pressure, heart rate, and breathing become erratic, making intensive care management far more complex.
Factors Affecting Survival
Clinical Predictors of Better Outcomes
Not every case follows the average. Some patients beat the odds. Heres what tends to tip the scales in their favor:
- Reactive pupils: If the pupils still respond to light, it usually means the brainstem is still functional.
- Early surgical decompression: Getting a craniectomy or hematoma evacuation within the first few hours can dramatically lower intracranial pressure.
- Younger age and fewer comorbidities: A healthy 30yearold has a better chance than an elderly patient with heart disease.
- Highquality ICU care: Continuous ICP monitoring, aggressive osmotherapy, and early mobilization matter.
Poor Prognostic Signs
Things that usually signal a grim outlook include:
- Fixed, dilated pupils (often >80% mortality, per )
- Persistent decorticate positioning despite optimal medical management
- Severe hypoxia or hypotension before hospital arrival
RealWorld Snapshots
Imagine a 24yearold who survived a highspeed motorcycle crash. He arrived with decorticate posturing, but his pupils were reactive and surgeons performed an emergency craniectomy within two hours. He went on to regain limited use of his right arm a story that aligns with the roughly 37% survival figure.
Contrast that with a 68yearold who suffered a massive basal ganglia hemorrhage. He presented with decerebrate posturing, fixed pupils, and a rapid decline in blood pressure despite maximal ICU support. Unfortunately, his outcome reflected the lower 10% survival rate typical for decerebrate patterns.
Treatment Options Overview
Emergency Actions
First things first protect the airway, control intracranial pressure, and stabilize circulation. Common emergency measures include:
- Intubation with cervical spine protection
- Hypertonic saline or mannitol to draw fluid out of the brain
- Ventilation strategies that keep CO low enough to reduce ICP without causing vasoconstriction
Surgical Interventions
When imaging reveals a spaceoccupying bleed or swelling, neurosurgeons may perform:
- Decompressive craniectomy removing a portion of the skull to give the brain room to swell safely.
- Hematoma evacuation drilling out a clot thats pressing on critical structures.
- Ventriculostomy placing a drain to remove excess cerebrospinal fluid.
Rehabilitation and LongTerm Care
Surviving the acute phase is just the beginning. Physical therapy, occupational therapy, and speech-language pathology become the backbone of recovery. Families should also look into psychological support for both the patient and themselves the emotional toll can be huge. For families navigating complex long-term care options and insurance questions after a severe brain injury, resources on Exondys 51 insurance provide a useful example of how patient assistance and coverage pathways can affect recovery planning.
Bottom Line Takeaway
Decorticate posturing carries a roughly 37% survival rate, significantly higher than the ~10% seen with decerebrate posturing. Yet those numbers are averages; individual outcomes hinge on factors like pupil reactivity, rapid medical response, and the exact location of brain injury. Understanding the difference between these postures helps you ask the right questions of your medical team and gives you a clearer picture of what the road ahead might look like.
Above all, remember that statistics are a guide, not a verdict. Early, aggressive treatment can move a patient closer to the higher end of the survival curve, and supportive rehabilitation can make a world of difference in quality of life.
Expert Sources & Trust
To keep the information trustworthy, this article draws on peerreviewed medical literature and statements from leading neurology centers. Youll find data from the StatPearls collection, the Cleveland Clinics braininjury guidelines, and several systematic reviews published in journals such as Neurosurgery and Critical Care Medicine. Where possible, weve highlighted the most uptodate findings because accurate, current knowledge is the backbone of good care.
If you ever find yourself standing at the crossroads of confusion and fear, remember: asking clear, informed questions and advocating for timely, specialized care can shift the odds in your favor. Youre not alone in this journey, and theres a community of clinicians and families ready to walk alongside you.
FAQs
What is the survival rate for decorticate posturing?
Approximately 37% of patients who develop decorticate posturing after a brain injury survive long term, though this rate varies with other clinical factors.
How does decorticate posturing differ from decerebrate posturing in prognosis?
Decorticate posturing indicates injury above the red nucleus and has a better survival rate (~37%) compared to decerebrate posturing (~10%), which signals deeper brainstem damage.
Which brain areas are affected in decorticate posturing?
Decorticate posturing results from damage above the red nucleus, mainly involving the corticospinal tract from the motor cortex to the spinal cord.
What factors improve survival odds in decorticate posturing?
Better outcomes are associated with reactive pupils, early surgical decompression, younger age, fewer comorbidities, and rapid receipt of high-quality ICU care.
Why is decerebrate posturing associated with worse outcomes?
Decerebrate posturing suggests brainstem injury, leading to loss of protective reflexes and autonomic instability, both of which significantly increase mortality risk.