If you or someone you love is battling COPD, the right ventilator can feel like a lifeline. In a nutshell, there are two families youll hear about most often: noninvasive ventilators that work through a mask, and invasive ventilators that require a tube placed in the airway. Each has its own strengths, weaknesses, and ideal moments to step in.
Choosing wisely isnt just about the machinesits about comfort, safety, and staying as independent as possible. Below youll find a friendly, downtoearth guide that walks you through every COPD ventilator type, the settings that matter, the realworld outcomes you might expect, and a few practical tips you can start using right now.
Why Ventilation Matters
During a severe COPD flareup, the lungs struggle to move enough air in and out. That can lead to dangerous levels of carbon dioxide, low oxygen, and an overwhelming feeling of breathlessness. Mechanical ventilation steps in to give the respiratory muscles a break and restore proper gas exchange.
Guidelines from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the American Thoracic Society recommend starting with noninvasive positivepressure ventilation (NPPV) whenever possible, because it carries fewer complications than invasive ventilation. , early NPPV can reduce intubation rates by up to 30%.
NonInvasive Options
What Is NonInvasive PositivePressure Ventilation?
Noninvasive ventilation (NIV) delivers air through a snug face or nasal mask. The most common machines youll see in hospitals or at home are branded as BiPAP, CPAP, or portable devices like the Respironics Trilogy.
Key Settings for COPD
- Inspiratory Positive Airway Pressure (IPAP): Usually set between 1020cmHO to support each breath.
- Expiratory Positive Airway Pressure (EPAP or PEEP): Typically 58cmHO, helping keep the airways open without overinflating the lungs.
- Backup Respiratory Rate: 1216 breaths per minute, ensuring a steady rhythm if the patients own breathing slows down.
Pros & Cons
Pros: No surgical airway, lower infection risk, and patients can usually speak, eat, and even read while on the machine. Cons: Mask leaks can be noisy, and some patients find the mask uncomfortable, especially after several hours.
How to Set PEEP in COPD (PEEP in COPD ventilation)
1. Start at 5cmHO.
2. Observe oxygen saturation and comfort.
3. If oxygen improves without signs of lung overdistension (e.g., high plateau pressures), increase by 12cmHO increments up to 8cmHO.
4. Recheck arterial blood gases after each change.
RealWorld Example
Emily, 62, was admitted with a COPD exacerbation. Her doctors started her on BiPAP with IPAP=15cmHO and EPAP=6cmHO. Within 90 minutes her blood CO dropped from 68mmHg to 55mmHg, and she avoided intubation altogether. Stories like Emilys illustrate why NIV is often the first line of defense.
When NonInvasive Isnt Enough
If the blood gas numbers stay stubbornly abnormalpH below 7.25 or CO above 60mmHgafter an hour or two of optimal NIV, its time to consider invasive ventilation. The decision isnt easy, but it can be lifesaving.
Invasive Options
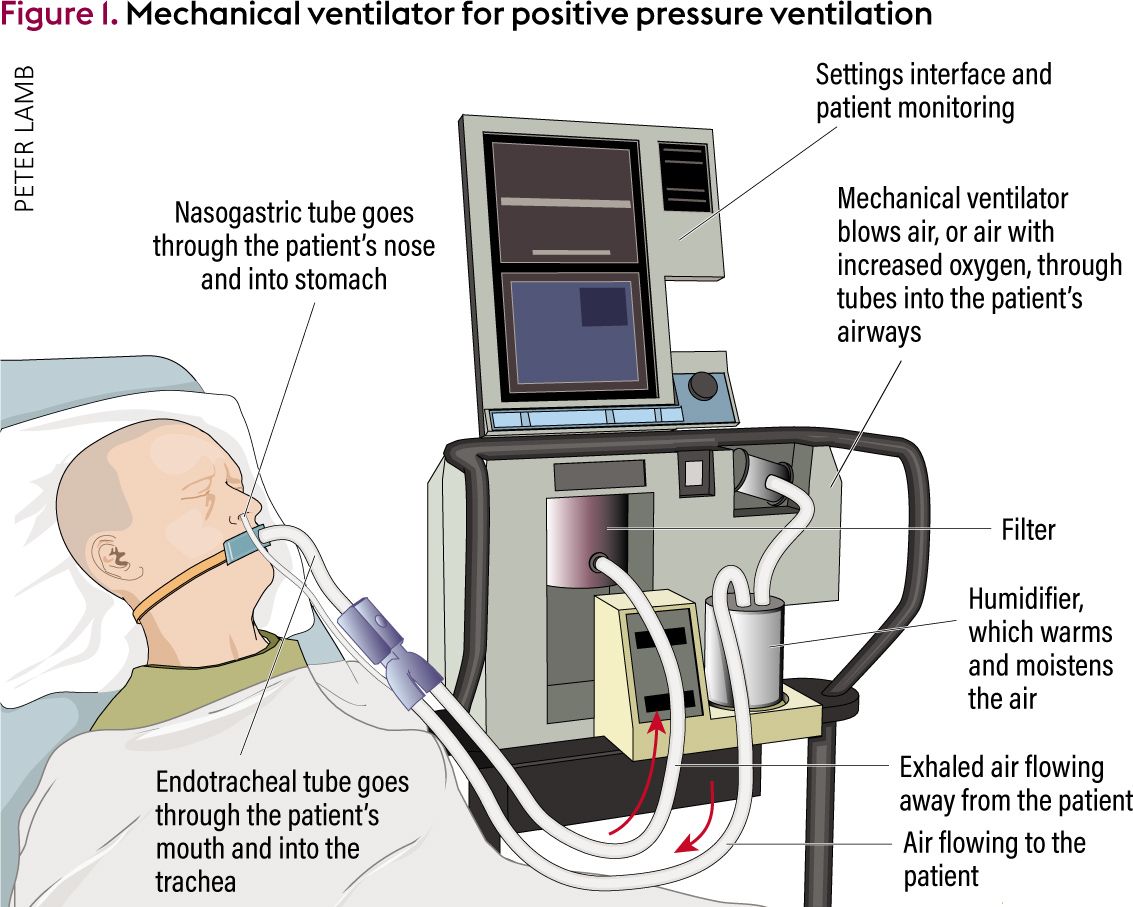
What Is Invasive Mechanical Ventilation?
Invasive ventilation means a tube (endotracheal or tracheostomy) is placed directly into the airway. The machine then takes over all or part of the breathing work. Its the most aggressive form of support, used when noninvasive strategies fail or when the patient cant protect their airway.
Ventilator Modes Most Common in COPD
- VolumeControl Ventilation (VCV): Guarantees a set tidal volume, useful for precise control.
- PressureTargeted (PressureControl) Ventilation: Limits peak pressure, protecting the lungs from barotrauma.
- Synchronized Intermittent Mandatory Ventilation (SIMV): Allows spontaneous breaths between mandatory cycles, encouraging weaning.
Survival Rate After Intubation (survival rate after intubation COPD)
Metaanalyses published in 2023 show a 30day survival of roughly 30%45% for COPD patients who require intubation, depending on age, comorbidities, and how quickly the underlying cause is treated. A study in the Journal of Critical Care highlighted that early initiation of lowtidalvolume ventilation improves those odds.
Invasive Settings for COPD
Typical starting points:
- Tidal Volume: 68mL per kilogram of ideal body weight.
- PEEP: 510cmHO, titrated to improve oxygenation without causing hyperinflation.
- Plateau Pressure: Keep below 30cmHO to reduce barotrauma risk.
- Permissive Hypercapnia: Allow a higher CO level (up to 55mmHg) if pH remains above 7.20, easing the burden on stiff lungs.
Case in Point
Mark, 71, arrived with severe acidosis (pH=7.18). After failed NIV, clinicians performed a rapid sequence intubation and set the ventilator to volumecontrol with a tidal volume of 7mL/kg, PEEP=8cmHO. Within 48hours his pH rose above 7.35, and he was successfully weaned off the ventilator. Real cases underscore that invasive support, when timely, can be a bridge to recovery.
Choosing the Right
DecisionMaking Flowchart
- Acute exacerbation? Start with NPPV.
- Is NPPV working? Look at ABG after 12hours. If pH<7.25 or CO>60mmHg, move to invasive ventilation.
- Longterm needs? Evaluate homeventilator options or consider tracheostomy for endstage COPD ventilator support.
PatientCentered Factors
Age, overall health, and personal goals matter as much as the numbers. Some patients prioritize remaining at home, even if that means using a portable BiPAP for months. Others feel more comfortable with a definitive airway if the disease is very advanced. Similar to cystic fibrosis patients who rely on cystic fibrosis airway clearance techniques for lung mucus management, COPD patients benefit greatly from airway clearance and chest physiotherapy practices tailored to their breathing needs.
Life Expectancy on Ventilator (life expectancy on ventilator COPD)
Studies suggest that for endstage COPD patients who transition to longterm home ventilation, median survival ranges from 1 to 3years, heavily influenced by comorbidities such as heart failure. Public health data emphasize that quality of life often improves when the ventilator is tailored to the individuals comfort needs.
Testimonial
Laura shared, When my doctor explained the difference between a hospitalgrade machine and the portable one we could use at home, I felt empowered. We chose a home BiPAP, and the freedom to sit on the porch again meant everything. Real stories like Lauras remind us that the right choice is deeply personal.
Managing Risks
Common Complications & Prevention
| Complication | Prevention Tip | Reference |
|---|---|---|
| VentilatorAssociated Pneumonia | Elevate head of bed 3045, use subglottic suction | ATS 2022 |
| Barotrauma | Keep plateau pressure <30cmHO, monitor chest Xray | UpToDate |
| Mask Skin Breakdown (NIV) | Rotate mask, apply silicone pads, adjust strap tension | ResMed Clinical Guide |
Monitoring & FollowUp
Daily arterial blood gases (or at least capillary CO checks) let you see if the ventilator settings are hitting the sweet spot. Keep an eye on:
- SpO>90% (or patientspecific target)
- pH>7.35 for weaning readiness
- Respiratory rate<25 breaths/min
When the numbers stabilize, you can start a gentle weaning protocolreduce pressure support by 12cmHO every 1224hours while watching for fatigue.
QuickCheck List for Caregivers
- Verify alarm thresholds each shift.
- Inspect tubing for leaks or kinks.
- Record a comfort score (010) from the patient.
- Log nightly sleep qualitypoor sleep often signals a need to adjust settings.
Helpful Resources
Want to dive deeper? These trustworthy sources keep the information uptodate:
- the gold (pun intended) standard for treatment pathways.
- American Thoracic Society (ATS) clinical practice statements on mechanical ventilation.
- UpToDates chapter on Mechanical ventilation in patients with chronic obstructive pulmonary disease.
- MedicalNewsTodays explainer on home ventilators for COPD patients.
Conclusion
Choosing the right COPD ventilator type isnt a onesizefitsall decision. Noninvasive options give you comfort and freedom, while invasive ventilation steps in when the lungs need a fulltime rescue. Understanding the key ventilator settingsPEEP, pressure support, tidal volumehelps you and your healthcare team finetune therapy for the best possible outcomes.
Remember, its okay to ask questions, voice concerns, and involve loved ones in the conversation. If youre facing a COPD flareup, start by discussing noninvasive options with your doctor; if the situation escalates, know that invasive support can be a bridge to recovery when used promptly and wisely. We hope this guide clears the fog around COPD ventilators and empowers you to make informed, confident choices.
FAQs
What are the main COPD ventilator types?
The two primary types are non‑invasive ventilators (delivered via a mask, e.g., BiPAP or CPAP) and invasive ventilators (requiring an endotracheal tube or tracheostomy).
When should a patient move from non‑invasive to invasive ventilation?
If arterial blood gases remain abnormal after 1‑2 hours of optimal non‑invasive support—specifically pH < 7.25 or CO₂ > 60 mmHg—transition to invasive ventilation is usually indicated.
What are the key pressure settings for COPD patients on NIV?
Typical starting points are IPAP 10‑20 cmH₂O, EPAP (PEEP) 5‑8 cmH₂O, and a backup respiratory rate of 12‑16 breaths per minute, adjusted based on comfort and blood‑gas results.
How does permissive hypercapnia help during invasive ventilation?
Allowing a higher CO₂ level (up to ~55 mmHg) while keeping pH > 7.20 reduces the risk of barotrauma and lung over‑distension in stiff COPD lungs.
What is the typical survival rate after intubation for COPD patients?
Recent meta‑analyses show a 30‑day survival of roughly 30 %–45 % for COPD patients who require invasive ventilation, depending on age, comorbidities, and timeliness of treatment.