Quick answer: an MRI can spot a stroke within minutes of it happening, and the changes stay visible for weeks or even monthsfar longer than a CT scan. Getting the right imaging fast can be the difference between a full recovery and lasting brain injury.
Why MRI Matters
When you or a loved one experiences sudden weakness, trouble speaking, or vision changes, the clock starts ticking. Doctors need the most accurate picture of what's happening inside the brain, and that's where stroke detection MRI shines. Unlike a CT scan, which is great at spotting bleeding, MRI is incredibly sensitive to the early, subtle changes of an ischemic stroke.
Early Tissue Changes
Within just five to ten minutes after a blockage, a diffusion-weighted imaging (DWI) sequence shows a bright spot where water molecules are trapped. This hyperintensity is like a neon sign flashing that something is wrong, while a CT might still look perfectly normal. Studies from the confirm that DWI detects over 90% of acute ischemic strokes.
Differentiating Stroke Types
MRIs don't just say something's wrong; they tell you what is wrong. With sequences such as FLAIR, T2, and susceptibility-weighted imaging (SWI), doctors can tell if the stroke is caused by a clot (ischemic) or bleeding (hemorrhagic). This distinction is crucial because the treatments are worlds apartclot-busting drugs for ischemic strokes, and surgery or careful monitoring for hemorrhagic ones.
Detecting Mini-Strokes
Ever heard of a mini-stroke or TIA (transient ischemic attack)? It often leaves no trace on a CT, but an MRI can catch tiny DWI lesions that explain the symptoms. In one real-world story, a 58-year-old man thought his brief numbness was nothing, but his MRI revealed a small ischemic spot that prompted immediate antiplatelet therapy, preventing a larger event later.
Long-Term Monitoring
After the acute phase, MRI remains valuable. It can track scar tissue, monitor for new lesions, and help doctors decide on secondary prevention strategies. The changes can be followed for months, giving a clear roadmap of healingor warning signs that need attention. In some neurological and genetic syndromes, such as atypical Rett syndrome, monitoring brain changes and neurological symptoms is a similarly complex task that benefits from advanced imaging and standardized criteria.
MRI vs CT
Both MRI and CT have their strengths, and the choice often depends on timing, availability, and the specific question doctors need answered.
Speed and Access
CT scans are quickoften done in under 10 minutesand are available in virtually every emergency department. MRI takes longer (2045 minutes) and may not be on hand in every hospital, especially after hours. That's why many protocols start with a CT to rule out a bleed, then move to MRI if the CT is negative but symptoms persist.
Radiation vs No Radiation
CT uses ionizing radiation, which is a concern for younger patients and repeated scans. MRI uses magnetic fields and radio wavesno radiationmaking it a safer choice for follow-up imaging.
Contrast Use
Both modalities can use contrast agents. Iodine-based contrast in CT helps highlight blood vessels, while gadolinium-based contrast in MRI adds detail to the blood-brain barrier and can differentiate newer from older hemorrhages. However, a non-contrast MRI is usually enough for detecting acute ischemia.
Detecting Hemorrhage
CT excels at spotting acute bleeding because fresh blood appears bright. MRI can also detect hemorrhage, especially with SWI, which can even age a bleed based on how the blood products appear. So, each has a role: CT for rapid bleed detection, MRI for detailed tissue characterization. For diseases with varying neurological presentations, such as Rett syndrome criteria are used alongside imaging and clinical findings to guide diagnosis and management.
| Time Post-Onset | MRI Sequence | Typical Findings | CT Visibility |
|---|---|---|---|
| <30min | DWI | Bright spot (restricted diffusion) | Often negative |
| 124hr | DWI + FLAIR | Emerging edema, fogging | May show early bleed |
| 37days | FLAIR, T2 | Established infarct, peak edema | Hypodensity appears |
| >2weeks | T2, SWI | Chronic gliosis, hemosiderin | Scar appears as hypodensity |
Getting the Scan
Feeling nervous about an MRI? Trust me, the process isn't as sci-fi as you might imagine. Here's a friendly walkthrough.
Before the Scan
- Remove metalwatch out for piercings, jewelry, or hair clips.
- If you have implants (pacemaker, certain cochlear implants), let the tech know; some are MRI-compatible, others aren't.
- No fasting needed, but a light snack can keep you from feeling faint.
During the Scan
The machine makes a series of loud knocks and hums, almost like a heavy-duty blender. You'll lie on a sliding table; a technician will guide you into a narrow tunnel. Staying still is keythink of it as a quick, still-as-a-statue meditation. If you're claustrophobic, ask about an open-MRI system or a mild sedative.
After the Scan
Results usually come back within 24 hours. You'll get a copy of the images if you ask, and the radiologist will write a report that your neurologist will discuss with you. Don't hesitate to ask for clarificationyour health, your questions.
Contrast Choices
Do you need contrast for a stroke MRI? In most cases, no. Non-contrast sequences (DWI, ADC, FLAIR) are enough to spot acute ischemia. Contrast becomes useful when doctors want to see the blood vessels more clearly (MRA) or suspect a tumor or active inflammation.
When to Use Gadolinium
- Assessing blood-brain barrier disruption (e.g., after a subacute hemorrhage).
- Getting high-resolution MRA to visualize arterial blockages without an invasive angiogram.
- Investigating lesions that might mimic stroke, such as demyelinating disease.
Risks and Benefits
| Aspect | Non-Contrast MRI | Contrast-Enhanced MRI |
|---|---|---|
| Safety | No gadolinium exposure | Rare allergic reactions; caution in severe kidney disease |
| Information | Detects diffusion changes only | Shows vessel anatomy, active inflammation, and blood-brain barrier status |
| Cost/Time | Faster, cheaper | Longer scan, higher cost |
Reading the Images
Even if you're not a radiologist, knowing what the radiologist looks for can demystify the report.
Key Sequences Explained
- DWI (Diffusion-Weighted Imaging): Bright spots = recent restriction of water movementacute stroke.
- ADC (Apparent Diffusion Coefficient) Map: Dark areas confirm true restriction; bright areas suggest pseudo-restriction.
- FLAIR (Fluid-Attenuated Inversion Recovery): Highlights edema and later-stage infarcts; lesions appear bright against suppressed CSF.
- SWI (Susceptibility-Weighted Imaging): Sensitive to blood productsgreat for spotting microbleeds or hemorrhagic transformation.
- MRA (Magnetic Resonance Angiography): Noninvasive vascular map showing which arteries are blocked.
Simple Cheat Sheet
Think of the brain like a city. DWI shows traffic jams (blocked roads) instantly. FLAIR reveals the smoke after the fire has started. SWI spots the tiny sparks of a hidden blaze. MRA is the overhead drone view of the whole road network.
Real-World Cases
Case 1: Lightning-Fast Detection
Emily, 42, felt a sudden loss of speech while cooking. She arrived at the ER within an hour. A CT was clean, but the neurologist ordered an MRI. Within 8 minutes of symptom onset, DWI showed a bright spot in the left frontal lobe. She received clot-busting therapy just in time, and her speech returned fully within days. , early MRI detection dramatically improves outcomes for eligible patients.
Case 2: The Hidden TIA
Mark, 58, experienced a fleeting weakness in his right arm that resolved in five minutes. He brushed it off until his wife urged a doctor's visit. CT was normal, but an MRI revealed a tiny DWI lesion in the internal capsuleevidence of a mini-stroke. This finding led to starting antiplatelet medication and lifestyle changes, likely preventing a larger stroke later that year.
Experience Matters
These stories underline why we, as patients and caregivers, should advocate for the most sensitive imaging available when stroke symptoms appear. It's not just about technology; it's about giving your brain the best chance to heal. Similarly, for complex or rare neurological conditions, understanding the Rett syndrome types or related criteria can guide families and clinicians to better care pathways.
Putting It All Together
So, what's the bottom line? If a stroke is suspected, an MRI is the gold standard for early detection, especially for ischemic strokes. It shows changes in minutes, stays visible for weeks, and informs the precise treatment pathway. CT still has a critical rolerapid bleed detection and universal availabilitybut MRI follows up to confirm the diagnosis and guide long-term care.
Here's a quick recap:
- Speed matters: Get any brain imaging ASAP.
- Use MRI when possible: It catches strokes earlier and more accurately than CT.
- Contrast isn't always needed: Noncontrast MRI is sufficient for most acute cases.
- Ask questions: Understanding the report empowers you to participate in treatment decisions.
Conclusion
When every second counts, stroke detection MRI offers the sharpest eyes we have to see what's happening inside the brain. Whether you're dealing with a sudden, terrifying symptom or trying to understand a mini-stroke that slipped by unnoticed, the right imaging can be life-changing. Talk to your healthcare provider about getting an MRI if stroke is on the tabledon't settle for just a scan when you can have the most detailed picture possible.
We'd love to hear from you: Have you or a loved one gone through stroke imaging? What questions still linger? Drop a comment below, share your story, or ask anything you're unsure about. Together we can turn uncertainty into confidence.
FAQs
What is the main difference between colorectal and colon cancer?
Colorectal cancer refers to any malignant tumor that starts anywhere from the cecum to the rectum, while colon cancer is a subset that originates only in the colon.
How do symptoms of colon cancer differ from rectal cancer?
Both can cause blood in stool and bowel changes, but rectal cancer often leads to rectal bleeding and may require additional pelvic symptoms, whereas colon cancer symptoms may be milder and include occasional mucus or anemia.
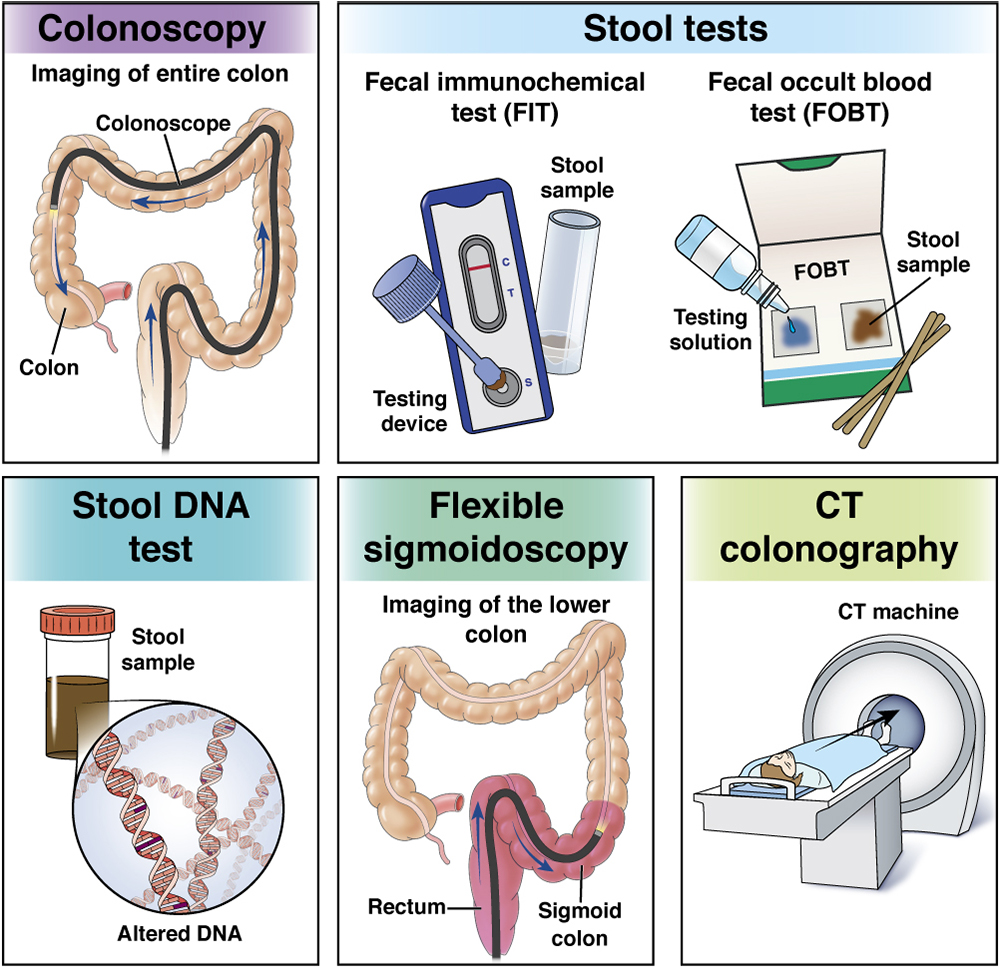
Which screening tests are recommended for detecting colorectal vs colon cancer?
Colonoscopy is the gold‑standard for both, but FIT (fecal immunochemical test) and CT colonography are also used, especially when a full colonoscopy isn’t possible.
What are the typical treatment approaches for colon cancer compared to rectal cancer?
Colon cancer usually involves surgical removal (colectomy) followed by chemotherapy if needed. Rectal cancer often requires neoadjuvant chemoradiation before surgery to shrink the tumor.
What is the “worst type” of colon cancer and how does it affect prognosis?
High‑grade, poorly differentiated tumors—especially signet‑ring cell carcinoma—are considered the most aggressive form, leading to faster spread and lower survival rates.