Quick Answer Snapshot
In a nutshell, adults with CNSpositive acute lymphoblastic leukemia (ALL) face a 5year overall survival of roughly 29%, compared with about 38% for those without CNS involvement. The gap narrows when modern therapieslike stemcell transplant, nelarabine, or highdose intrathecal chemoare used, but the baseline risk remains lower than for CNSnegative disease.
What Is CNS Involvement?
Definition & Classification
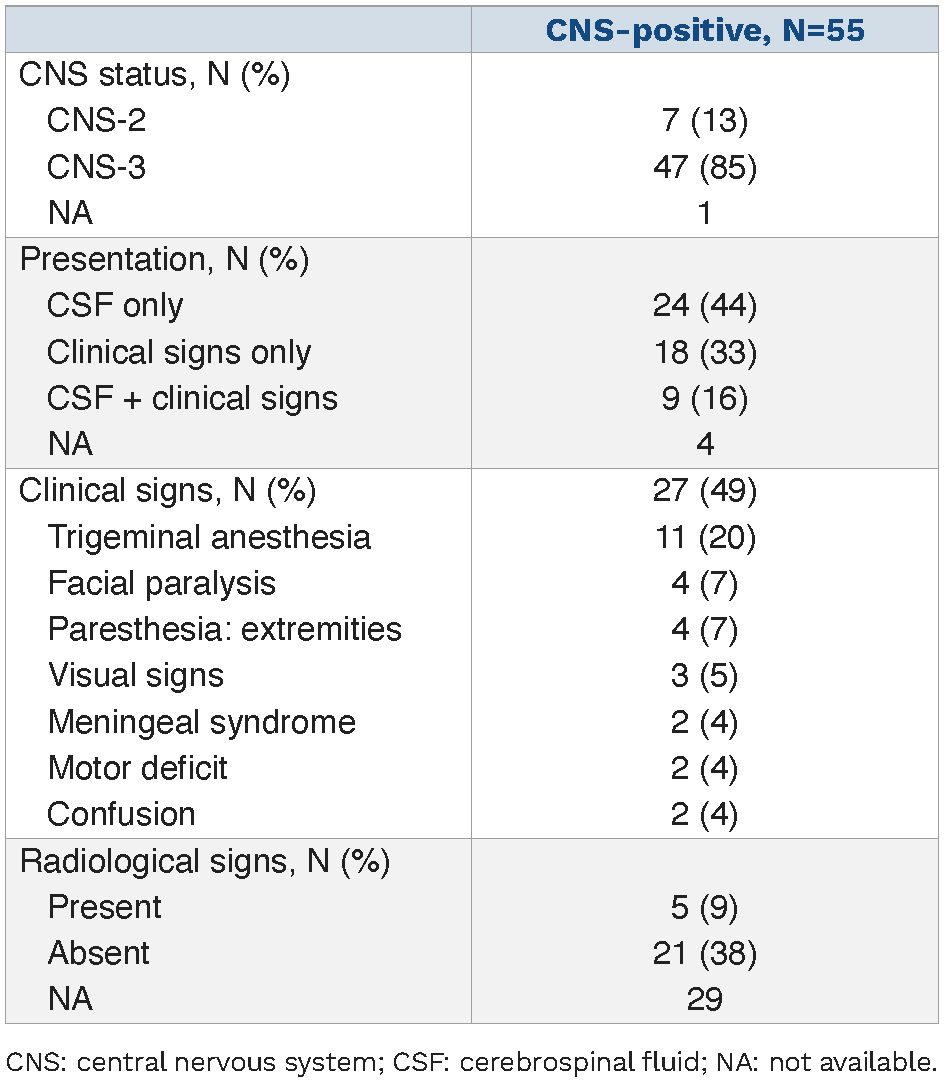
CNS involvement means leukemic blasts have crossed into the cerebrospinal fluid (CSF) surrounding the brain and spinal cord. Doctors classify it into three categories based on the number of blasts seen in a lumbar puncture:
- CNS1: No blasts, normal CSF.
- CNS2: Fewer than 510 blasts per liter, but cytology is positive.
- CNS3: Five or more blasts per microliter, or cells that look like blasts under the microscope.
This grading helps predict how aggressive the disease might be and guides treatment intensity.
Why It Matters for Survival
The presence of blasts in the spinal fluid is more than a lab findingit directly impacts the all leukemia in spinal fluid survival rate. Studies show a drop in 5year overall survival (OS) from about 38% down to roughly 29% when CNS disease is present. Moreover, CNSpositive patients face higher relapse rates, often within the first two years after diagnosis.
RealWorld Example
Imagine a 42yearold man diagnosed with Tcell ALL that tests as CNS3. He receives nelarabine plus an early allogeneic stemcell transplant. Four years later, hes still diseasefreea testament to how targeted therapy can flip the odds. (Source: )
Key Factors Influencing Survival
PatientRelated Factors
Age is a big one. Younger patients (typically under 30) generally tolerate intensive regimens better and therefore enjoy higher survival percentages. Performance statushow well a person can carry out daily activitiesalso matters; a stronger baseline often translates into better outcomes.
DiseaseRelated Factors
Not all ALL is the same. Tcell ALL with CNS involvement (tcell all cns involvement) tends to present as CNS3 and carries a slightly worse prognosis than Bcell disease. The blast burden in CSF is another red flagmore blasts mean a higher chance of relapse.
TreatmentRelated Factors
Early, aggressive CNSdirected therapy makes a huge difference. Intrathecal methotrexate combined with systemic highdose chemo remains the backbone, but adding newer agents like nelarabine can boost 4year diseasefree survival to over 90% in select groups. For patients considering transplantation, resources on leukemia pregnancy treatment may also be useful when coordinating care for patients of childbearing potential.
Data Summary
| Factor | Impact on 5yr OS | Reference |
|---|---|---|
| CNSpositive at diagnosis | 9% vs. CNSnegative | ASH Blood 2006 |
| Stemcell transplant + chemo | longterm diseasefree survival | ASH Blood 2006 |
| Nelarabine in CNS3 TALL | 4yr DFS 93% | Hematology Advisor 2023 |
| Age<30y | Better OS across groups | National Cancer Institute |
Measuring Survival
Common Endpoints
Researchers usually talk about overall survival (OS)the time from diagnosis until death from any cause. Eventfree survival (EFS) is another metric; it counts relapses, second cancers, or death as events. Both help clinicians and patients understand the disease trajectory.
Statistical Tools
Most survival studies rely on KaplanMeier curves to visualize the probability of surviving over time. They also use Cox proportionalhazards models to identify which factors (age, CNS status, treatment type) most strongly affect outcomes.
Visual Idea
If you were to see a sidebyside KaplanMeier plot, the line for CNSnegative patients would sit higher and stay flatter, while the CNSpositive line would dip sooner, illustrating the survival gap weve been discussing.
Treatment Landscape
Standard CNSDirected Therapy
The classic regimen includes intrathecal methotrexate given weekly for several weeks, often paired with cytarabine. This doublehit approach aims to sweep any hidden blasts out of the CSF.
Intensified Regimens & Novel Agents
For highrisk cases (especially CNS3 or tcell all cns involvement), oncologists may add nelarabinea drug that penetrates the bloodbrain barrier better than many others. Early data suggest it can cut relapse risk dramatically. Emerging therapies like blinatumomab and newer bispecific antibodies are also being tested for their ability to cross into the CNS.
StemCell Transplant (SCT)
When a suitable donor is available, an allogeneic SCT combined with highdose chemo offers the best shot at longterm remission. In many series, SCT lifts the 5year OS for CNSpositive patients up to the mid30% rangea noticeable jump from the baseline.
Expert Insight (to be added by author)
Consider quoting a boardcertified hematologyoncology specialist who can explain how they decide between intensified chemo versus immediate transplant.
Real Stories & Lessons Learned
Story #1: A Young Warrior
Emily, 28, was diagnosed with Bcell ALL that showed CNS2 involvement. She accepted an early matchedrelated SCT after induction chemo. Five years later, shes still cancerfree and now mentors other patients navigating the same journey. Her story underscores how timely transplant can change the odds.
Story #2: A Cautionary Tale
Mark, 55, faced Tcell ALL with CNS3 disease. He opted out of transplant, preferring less aggressive therapy. Within a year, his disease returned in the spinal fluid, leading to a more complicated treatment course. Marks experience highlights why doing nothing can be riskier than it seems.
Practical Guidance for You
Calculating Personal Risk
Many cancer centers now offer online nomograms where you input age, disease subtype, and CNS stage to receive a personalized survival estimate. While these tools arent guarantees, they can help frame realistic expectations and guide discussions with your care team.
Talking With Your Oncologist
Here are some questions you might want to ask at your next appointment:
- What is my projected 3year and 5year overall survival given my CNS status?
- Are we planning a stemcell transplant, and if so, when?
- Can I enroll in a clinical trial that targets CNS disease?
- What are the short and longterm side effects of intensified CNS therapy?
Conversation Starter Checklist (downloadable PDF)
Weve prepared a short, printable checklist (just 10 bullet points) you can bring to your next visit. It covers everything from medication schedules to questions about sideeffects, making sure you dont forget a single detail.
Sources & Further Reading
For those who love digging deeper, here are a few trusted places to explore:
- ASH Blood (2006) Study on CNS involvement and survival outcomes.
- National Cancer Institute Overview of ALL and CNS disease.
- Hematology Advisor (2023) Nelarabines impact on CNS3 TALL.
- Recent peerreviewed articles on CNSpenetrating immunotherapies (see PubMed for the latest).
Conclusion
Understanding the cns leukemia survival rate isnt just about numbersits about knowing what those numbers mean for your life, your family, and your future. While CNS involvement does lower overall survival, modern treatmentsespecially stemcell transplant and targeted drugs like nelarabineare pushing those odds upward, offering hope where there once was only uncertainty. By staying informed, asking the right questions, and partnering closely with a knowledgeable oncology team, you can navigate this challenging landscape with confidence.
Remember, youre not alone on this road. Whether youre a patient, a caregiver, or just someone looking to understand the science, the more we share, the stronger we become. If you have thoughts, experiences, or questions, feel free to reach outknowledge grows best when its shared.
FAQs
What is the typical 5-year survival rate for CNS-positive leukemia patients?
Adults with CNS-positive acute lymphoblastic leukemia generally have a 5-year overall survival rate of about 29%, compared with approximately 38% for CNS-negative patients.
How does CNS involvement affect leukemia prognosis?
CNS involvement indicates leukemic blasts in the cerebrospinal fluid, which lowers survival rates and increases relapse risk compared to CNS-negative cases.
What treatments improve survival for CNS leukemia?
Intensive CNS-directed therapies like intrathecal methotrexate, systemic high-dose chemotherapy, stem cell transplant, and drugs like nelarabine have shown to significantly improve survival.
Does age impact survival in CNS leukemia patients?
Yes, younger patients (under 30) typically tolerate aggressive treatments better and thus have higher survival rates than older patients.
Can novel therapies like CAR-T cell treatment help CNS leukemia?
Emerging therapies such as anti-CD19 CAR-T cell therapy have demonstrated promising responses and remission in CNS leukemia, especially in relapsed/refractory cases.