Below youll get straight answers to the questions that keep you up at night, plus realworld tips that actually work. Think of this as a friendly chat over coffee warm, honest, and full of the information you need right now.
Quick Overview
| Disorder | Type | How common in pregnancy | Key concern |
|---|---|---|---|
| Antiphospholipid syndrome (APS) | Clotting | 15% of highrisk pregnancies | Miscarriage, thrombosis |
| VonWillebrand disease (VWD) | Bleeding | 0.51% | Excessive bleeding at delivery |
| Sickle cell disease / Thalassemia | Hemoglobin | 0.10.3% (varies by ethnicity) | Fetal growth restriction |
| Gestational thrombocytopenia | Plateletlow | 710% | Usually mild, but must rule out ITP |
| Rare clotting defects (e.g., proteinC/S deficiency) | Clotting | <0.1% | High risk for placental clotting |
This snapshot shows that blood disorders in pregnancy range from fairly common (like gestational thrombocytopenia) to truly rare conditions. Knowing where you land on that spectrum helps you and your doctor craft a plan thats just right for you.
Common Disorders
Which bleeding disorders show up most often?
When it comes to bleeding, VonWillebrand disease (VWD) tops the list. Its an inherited problem where your blood doesnt cling together as well as it should, leading to heavy periods, nosebleeds, or, in pregnancy, added bleeding at delivery. The good part? Most women with VWD have mild symptoms that can be managed with medication like desmopressin when the big day arrives.
Platelet function disorders are rarer, but they do exist. If youve ever been told you have unexplained bruising or a low platelet count, its worth asking your OBGYN to check for an underlying platelet issue. offers a clear, patientfriendly overview of these conditions.
Which clotting disorders are most common?
Antiphospholipid syndrome (APS) is the headline act for clotting disorders in pregnancy. Its an autoimmune condition where your body creates antibodies that turn the bloods clotting gears up too high, endangering the placenta and increasing the risk of miscarriage. Studies from show that lowdose aspirin combined with lowmolecularweight heparin (LMWH) can dramatically improve outcomes.
Other common culprits include FactorV Leiden and deficiencies in proteinC or proteinS. These genetic quirks quietly raise your clotforming tendency, especially as pregnancy hormones naturally tilt the balance toward clotting. While theyre each individually rare, together they account for a noticeable slice of highrisk pregnancy cases.
Realworld snippet
Emma, 32, learned she had APS after two early losses. With a hematology consult at and a regimen of lowdose aspirin, she carried to 38weeks without complications. a patientshared story we hear often enough to remind us that proactive care works.
Risks & Complications
How do blood disorders raise the chance of miscarriage?
Think of the placenta as a delicate garden. In clotting disorders like APS, tiny clots can form inside the gardens irrigation system, choking off the flow of oxygen and nutrients to the growing baby. In bleeding disorders such as VWD, uncontrolled bleeding can lead to low blood volume for both mom and baby, creating a stressful environment that sometimes ends in loss.
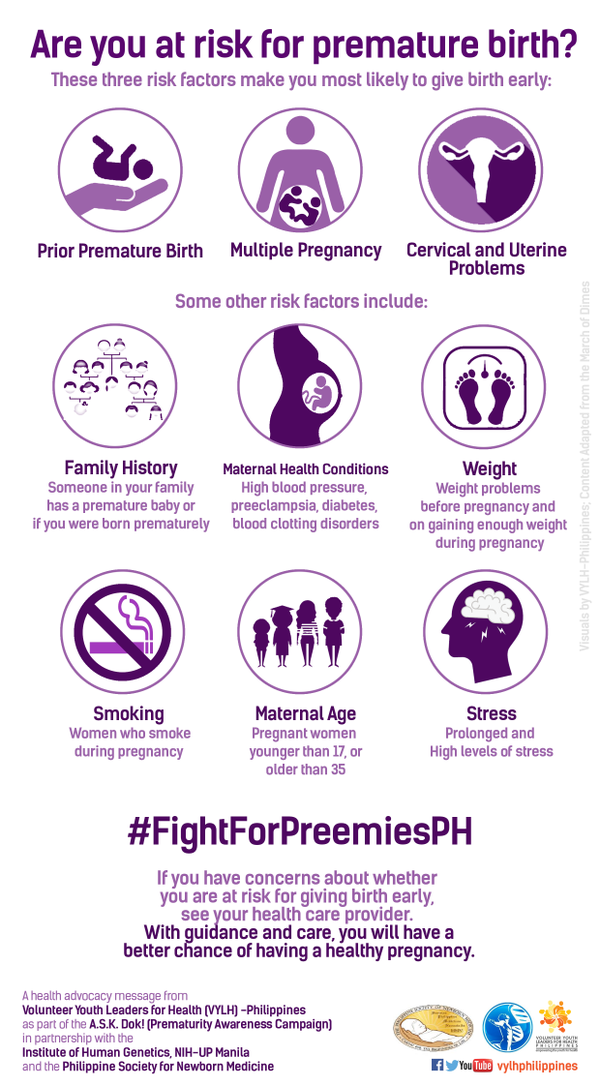
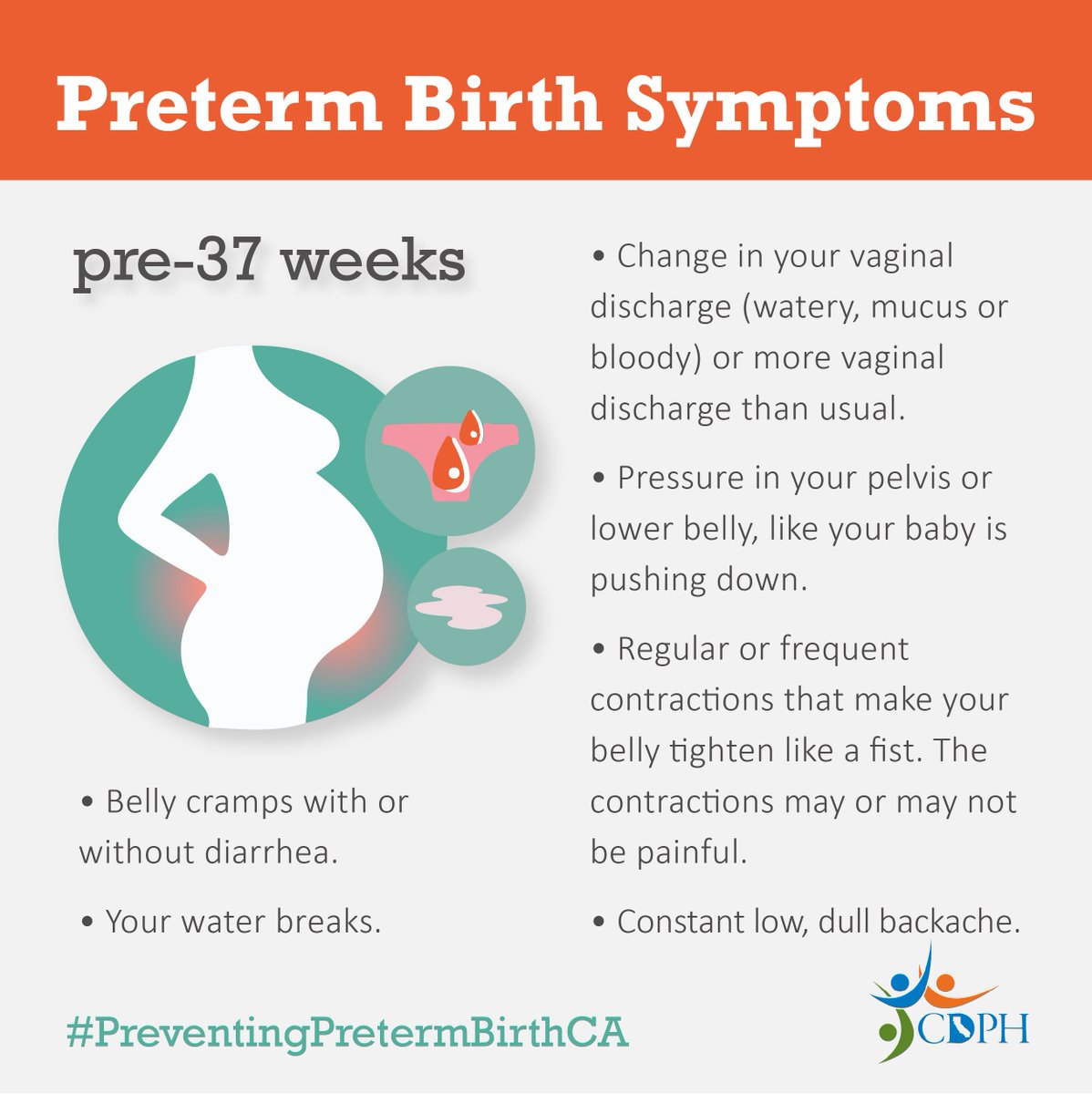
Which disorders lead to preterm birth and why?
When the placentas blood vessels are compromisedwhether by clotforming antibodies (APS) or by chronic anemia from sicklecell diseasethe babys growth slows. Doctors often recommend earlier delivery to keep the baby safe, which translates into preterm birth for many mothers. For more on common causes and strategies to prevent early delivery, read about premature birth causes and evidence around management.
Can a blood clotting disorder cause a stillbirth?
Its rare, but massive placental infarction (a large area of dead tissue due to blocked blood flow) can happen in severe clotting disorders, resulting in stillbirth. Prompt monitoring and anticoagulation therapy dramatically lower that risk, which is why early diagnosis is a lifesaver.
Risk Comparison Table
| Disorder | Miscarriage | Preterm birth | Placental clotting | Recommended monitoring |
|---|---|---|---|---|
| APS | High | High | Very High | Serial ultrasounds, LMWH |
| VWD | Low | Low | Negligible | FactorVIII/VWF levels |
| ProteinC deficiency | Moderate | Moderate | High | Anticoagulation protocol |
Diagnosis & Monitoring
Which tests should every pregnant woman with a suspected blood disorder get?
A thorough workup typically includes:
- Complete blood count (CBC) the baseline for anemia or thrombocytopenia.
- Coagulation panel (PT, aPTT) checks how fast your blood clots.
- Antiphospholipid antibody panel essential for diagnosing APS.
- VonWillebrand factor antigen and activity determines VWD severity.
- Genetic screens for sicklecell, thalassemia, FactorV Leiden, and MTHFR mutations (blood clotting disorder in pregnancy MTHFR).
How often should monitoring happen?
Think of monitoring as a series of checkpoints:
- Preconception or firsttrimester baseline: get all labs done before the 12week mark.
- Every 46weeks for highrisk conditions: especially if youre on aspirin or LMWH.
- Midtrimester growth scan: to ensure the babys developing as expected.
- Weekly checkins in the third trimester: if you have a clotting disorder or severe thrombocytopenia.
Resources you can download
For deeper dives, many universities host a free and an accompanying that break down the science into bitesize slides.
Treatment Options
What medication regimens are safe and effective?
Below are the most widely accepted treatments, backed by professional societies:
- Lowdose aspirin (4081mg daily): reduces placental clot formation in APS and other thrombophilias. Its considered safe throughout pregnancy.
- Lowmolecularweight heparin (LMWH): the goto anticoagulant for highrisk clotting disorders. It does not cross the placenta, so the baby stays safe.
- Desmopressin (DDAVP): used for mild VWD during labor to boost clotting factor levels.
- Iron & folic acid supplementation: essential for anemiarelated disorders, helping both mom and baby stay energized.
Can surgery ever be part of the plan?
Surgical interventions (like splenectomy) are rarely performed during pregnancy because the risks outweigh the benefits. If surgery is needed, doctors usually schedule it after delivery, unless a lifethreatening hemorrhage forces an emergency operation.
Everyday lifestyle tweaks that actually help
Medication is powerful, but small habits reinforce the treatment:
- Stay wellhydrated dehydration can increase clot risk.
- Move around every hour even a short walk around the house reduces stasis.
- Wear compression stockings if youre on anticoagulants.
- Track any new bruising, swelling, or unusual pain, and report it immediately.
- Keep all prenatal appointments; missing one can delay detecting a problem.
Stepbystep checklist
- Confirm your diagnosis with a hematology specialist.
- Set up a joint OBGYN plus hematology followup schedule.
- Start lowdose aspirin or LMWH as prescribed.
- Log daily symptoms (bleeding, leg swelling, shortness of breath).
- Work with your care team to create a birthplan that includes timing of medication pauses before labor.
Managing HighRisk Pregnancy
When should you consider a tertiarycare center?
If any of the following apply, its time to think bigger:
- Severe clotting disorder (e.g., APS with prior loss).
- Repeated miscarriages despite treatment.
- Fetal growth restriction diagnosed on ultrasound.
- Need for advanced fetal monitoring or neonatal intensive care.
These centers have maternalfetal medicine (MFM) teams who coordinate care between obstetricians, hematologists, and neonatologists a true dream team for your babys safety.
How does delivery planning differ?
Mode of delivery is guided by your blood disorder and how youre being medicated. For example, women on LMWH typically aim for a vaginal delivery if platelet counts are safe, but a scheduled Csection might be chosen if clotting risk is high or if we need to control the timing of medication pauses. If preterm delivery becomes likely because of placental issues, understanding preterm birth risks helps you and your team weigh timing and interventions.
Expert insight
Dr. L. Chen, a maternalfetal specialist at , notes, Coordinating care early with a hematologist reduces NICU stays by up to 30% across our highrisk cohort.
Trusted Resources & Further Reading
When youre ready to dig deeper, these sources are reliable, uptodate, and written for both patients and clinicians:
- Peerreviewed article: Congenital and Acquired Bleeding Disorders in Pregnancy (PMC)
- Downloadable
- Free
Conclusion
Pregnancy with a blood disorder can feel like walking a tightrope, but you dont have to do it alone. By recognizing the warning signs early, staying on top of regular monitoring, and embracing proven treatmentsfrom lowdose aspirin to LMWHyou give yourself the best possible chance for a healthy delivery. Remember, youre part of a team that includes your OBGYN, a hematology specialist, and often a maternalfetal medicine expert. Keep asking questions, trust the evidencebased guidance, and lean on the supportive community around you. Your journey is unique, but youve now got the knowledge to navigate it with confidence.
Whats your experience with blood disorders during pregnancy? Share your story in the comments, or drop us a question if something feels unclear. Were here for you, every step of the way.
FAQs
What are the most common blood disorders during pregnancy?
Common blood disorders in pregnancy include antiphospholipid syndrome (APS), von Willebrand disease (VWD), sickle cell disease, thalassemia, and gestational thrombocytopenia. Each varies in frequency and risk profile.
How do blood disorders affect pregnancy outcomes?
Blood disorders can increase risks such as miscarriage, pre-term birth, fetal growth restriction, and in severe cases stillbirth, mainly due to clot formation or bleeding complications in the placenta or mother.
What treatments are safe for managing blood disorders during pregnancy?
Safe treatments include low-dose aspirin and low-molecular-weight heparin (LMWH) for clotting disorders, desmopressin for von Willebrand disease, and iron plus folic acid supplements for anemia-related conditions.
How often should a pregnant woman with a blood disorder be monitored?
Monitoring typically starts with baseline labs before 12 weeks, followed by exams every 4-6 weeks for high-risk cases, a mid-trimester growth scan, and weekly check-ins in the third trimester if severe.
When should a pregnant woman with a blood disorder consider a tertiary care center?
Referral to a tertiary care center is advised for severe clotting disorders, repeated pregnancy losses despite treatment, fetal growth restriction, or when advanced fetal and neonatal intensive care is anticipated.