Understanding Neonatal Apnea
What is apnea in newborns?
Neonatal apnea is a temporary stop in breathing that lasts at least 20seconds, or a shorter pause accompanied by a drop in heart rate (bradycardia) or oxygen saturation. Its not a disease itselfmore like a symptom that tells us the babys breathing control needs a little extra help.
How common is it?
Apnea is especially common in preterm infants. Roughly 3040% of babies born before 34weeks experience at least one episode, while fullterm infants rarely have clinically significant pauses. Knowing the odds helps you stay alert without living in constant fear.
Why does it happen?
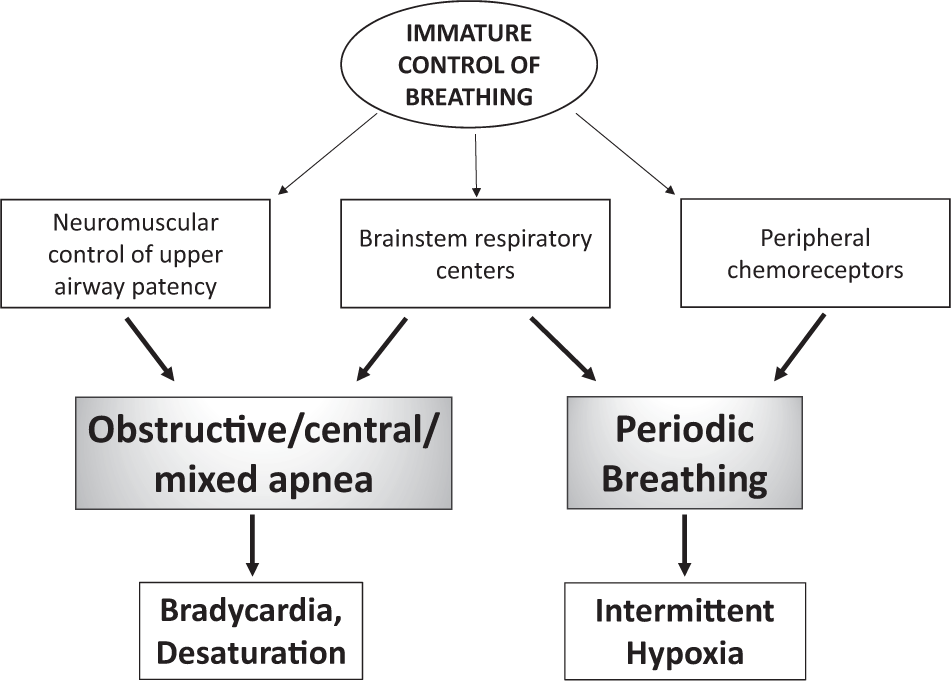
The newborns brainstem, which regulates breathing, is still maturing. Factors like infection, anemia, reflux, or certain medicines can tip the balance and trigger a pause.
Types of Apnea
Central apnea
Here the brain simply forgets to send a signal to the lungs. Its the most common form in very preterm babies because the respiratory center isnt fully wired yet.
Obstructive apnea
In this case the airway gets blockedoften by a soft tongue or by reflux that irritates the throat. The brain is trying to breathe, but the air cant get through.
Mixed (secondary) apnea
Mixed apnea starts as a central pause and then a blockage sneaks in, making it the trickiest to manage. Many NICUs track the proportion of mixed events because it guides treatment choices.
Causes and Risks
Prematurity
The earlier a baby arrives, the less developed the breathing centre is. Thats why apnea of prematurity guidelines stress close monitoring until around 36weeks postconceptual age.
Infections
Sepsis, meningitis, or even a mild viral infection can disturb the brains rhythm. Prompt antibiotics are often the first step in treatment.
Metabolic issues
Low blood sugar, anemia, or electrolyte imbalances can all provoke pauses. A quick blood panel usually clarifies whether any of these are at play.
Medications
Drugs such as morphine or benzodiazepines, sometimes given for pain or sedation, can depress the respiratory drive. Adjusting the dose or switching medication often resolves the problem.
Structural anomalies
Rarely, a laryngeal cleft or other airway malformation will cause obstructive episodes. Imaging studies can spot these early.
| Cause | Typical Treatment |
|---|---|
| Prematurity | Caffeine citrate, CPAP, gentle stimulation |
| Infection | Targeted antibiotics, supportive care |
| Anemia | Transfusion or iron supplementation |
| Reflux | Positioning, thickened feeds, possibly medication |
Recognizing Symptoms
Classic signs
A pause in breathing that looks like a silent gasp, followed by a bluish tint around the lips (cyanosis), a limp feeling, or a sudden drop in heart rate. Those are the redflag moments that need immediate attention.
Subtle cues
Sometimes the baby just looks a little jittery, arches their back, or seems unusually quiet after a pause. In the NICU, continuous cardiorespiratory monitors catch these microevents before parents notice.
Is a brief pause normal?
Short, isolated pauses are fairly common in the first few weeksespecially in pretermsbut anything lasting 20seconds or accompanied by desaturation isnt something to shrug off. When in doubt, call your neonatology team.
Diagnosing Apnea
Initial assessment
The doctor will start with a thorough physical exam, review the babys birth history, and ask about feeding patterns, medication exposure, and any recent infections.
Monitoring tools
Most NICUs use bedside cardiorespiratory monitors that log breathing, heart rate, and oxygen saturation. In complex cases, a sleep study (polysomnography) might be ordered, though its rare for newborns.
Lab work & imaging
A CBC, blood gas panel, and sometimes a cranial ultrasound help rule out anemia, metabolic disturbances, or brain injury. Chest Xrays can reveal lung congestion or structural problems.
Treatment Options
Treat the underlying cause
Whether its an infection, anemia, or reflux, fixing the root issue often stops the apnea. This is why a full workup is essential before jumping straight to medication.
Pharmacologic therapy caffeine citrate
Caffeine is the workhorse for apnea of prematurity. It stimulates the brains breathing centre and relaxes airway muscles, cutting pause frequency by 7080%. The typical dose starts at 20mg/kg (caffeine base), followed by a maintenance of 510mg/kg daily. Sideeffects are usually mildmaybe a faster heartbeat or a little jitterinessbut theyre far outweighed by the benefits.
Theophylline (alternative)
If a baby cant tolerate caffeine, theophylline is a backup. It works similarly but has a narrower therapeutic window, so blood levels need close monitoring.
Noninvasive respiratory support
Continuous Positive Airway Pressure (CPAP) keeps the airway gently open, especially useful for obstructive or mixed apnea. HighFlow Nasal Cannula (HFNC) delivers warm, humidified air at low pressures and is increasingly popular for milder cases.
Stimulation techniques
Before reaching for machines, many NICU nurses try a gentle rub on the babys back or feet. Its a simple, lowrisk way to restart breathing, and it works surprisingly well for brief central pauses.
Escalation intubation & ventilation
Only when apnea persists despite caffeine, CPAP, and stimulation do doctors consider a short course of mechanical ventilation. The goal is always to wean off as quickly as possible to avoid lung injury.
Surgical options (last resort)
In extremely rare cases where an anatomic blockage cannot be managed medically, procedures like tracheostomy or airway reconstruction may be discussed. These are highly specialized decisions made by a multidisciplinary team.
| Option | Pros | Cons |
|---|---|---|
| Caffeine citrate | Proven efficacy, easy administration | Possible tachycardia, jitteriness |
| Theophylline | Alternative when caffeine fails | Requires blood level monitoring |
| CPAP | Noninvasive, effective for obstructive apnea | Nasal skin irritation, need for equipment |
Benefits vs Risks
What treatment gives us
Effective therapy improves oxygenation, reduces NICU stay length, and protects the babys developing brain from recurrent hypoxic injury. That translates to better longterm neurodevelopmental outcomes.
Potential downsides
Every intervention carries a tradeoff. Caffeine can cause a faster heart rate; CPAP may leave tiny marks on the nose; and any medication can interact with other drugs the baby is receiving. Thats why neonatologists discuss the riskbenefit balance with families, ensuring youre part of every decision.
Shared decisionmaking
Think of it as a partnership. Your instincts, the babys daily patterns, and the medical teams expertise all blend together to find the safest, most comfortable plan.
When to Call
Redflag signs
If you see cyanosis, a heart rate below 80bpm, or more than two pauses in an hour, call the NICU immediately. Those are signals that the baby needs urgent intervention.
Immediate actions
First, gently stimulate the babyrub the back, tap the soles, or give a light shake if youre holding them securely. Then, if the baby doesnt resume breathing, call emergency services while someone else keeps the airway clear.
Followup plan
After an episode, the team will likely schedule repeat monitoringperhaps a bedside apnea monitor for a few days, then a checkup at 36weeks postconceptual age to assess whether caffeine can be tapered off. If anemia is suspected as a contributing factor, clinicians will evaluate and manage infant gastroenteritis or order a CBC to rule out pediatric anemia when appropriate.
Resources for Parents
Trusted medical sites
For deeper dives, sites like and the keep uptodate guidelines on neonatal apnea.
Parent support groups
Connecting with other families through the Premie Parents Network or the NICU Parent Alliance can turn anxiety into empowerment. Sharing storieslike Mias journey from a 28week birth to a thriving toddlerreminds us were not alone.
Printable cheatsheet
Consider downloading a onepage Apnea Action Plan that lists warning signs, emergency numbers, and the medication schedule. Having it on your fridge makes it easy to reference during a stressful moment.
Conclusion
Neonatal apnea can feel overwhelming, but thanks to evidencebased treatmentsespecially caffeine citrate and gentle breathing supportmost babies recover fully. Understanding the type of apnea, spotting the warning signs, and partnering with a knowledgeable NICU team gives you the best chance for a healthy start. Keep this guide handy, ask your doctor any questions that arise, and lean on parentfocused resources for ongoing support. Youre not just a caregiver; youre an advocate, and together we can ensure your little one gets the safe, nurturing environment they deserve.
FAQs
What is considered apnea in newborns?
Apnea in newborns is a pause in breathing that lasts at least 20 seconds, or a shorter pause accompanied by a drop in heart rate or oxygen saturation.
When should parents call the NICU for an apnea episode?
Call immediately if the baby shows cyanosis, a heart rate below 80 bpm, or experiences more than two pauses in an hour.
How does caffeine citrate help treat apnea of prematurity?
Caffeine stimulates the brain’s respiratory center and relaxes airway muscles, reducing the frequency of breathing pauses by about 70‑80%.
Is CPAP safe for newborns with obstructive apnea?
Yes, CPAP provides gentle, continuous pressure to keep the airway open and is a non‑invasive, effective option for many infants.
Can a brief pause in breathing be normal for a newborn?
Short, isolated pauses are common in the first weeks, especially for pre‑term babies, but any pause lasting 20 seconds or causing desaturation should be evaluated.