Lets cut to the chase: if you or a loved one is living with heart failure, finding out you also have anemia can feel like getting hit with a surprise plot twist. The good news is that this doublewhammy isnt a hopeless sentenceits a medical puzzle we can solve together. Below you'll learn why anemia shows up in heart failure, what it looks like, how it changes the odds of hospital visits or even survival, and which treatments actually make a difference.
Why It Happens
How Does Heart Failure Cause Anemia?
When the heart struggles to pump blood efficiently, it drags along a cascade of changes that end up stealing the bodys ability to make red blood cells. First, lower kidney perfusion cuts back on erythropoietina hormone that tells the bone marrow to crank out new cells. Then, chronic inflammation raises hepcidin levels, which lock iron away in storage cells where it can't be used. Add in common issues like poor nutrition, gastrointestinal bleeding from medication, and you have a perfect storm for low hemoglobin. These mechanisms are especially important in DI heart failure, which often involves complex interactions between heart function and other organ systems.
Data Snapshot
| Mechanism | Impact on Red Blood Cells |
|---|---|
| Reduced renal perfusion | Erythropoietin RBC production |
| Inflammation-driven hepcidin | Iron sequestration functional iron deficiency |
| GI bleeding (e.g., from anticoagulants) | Direct loss of iron & blood |
Studies show that about one-third of patients with chronic heart failure develop anemia, and that number climbs as the disease progresses.
Key Signs
What Are the Signs of Anemic Heart Failure?
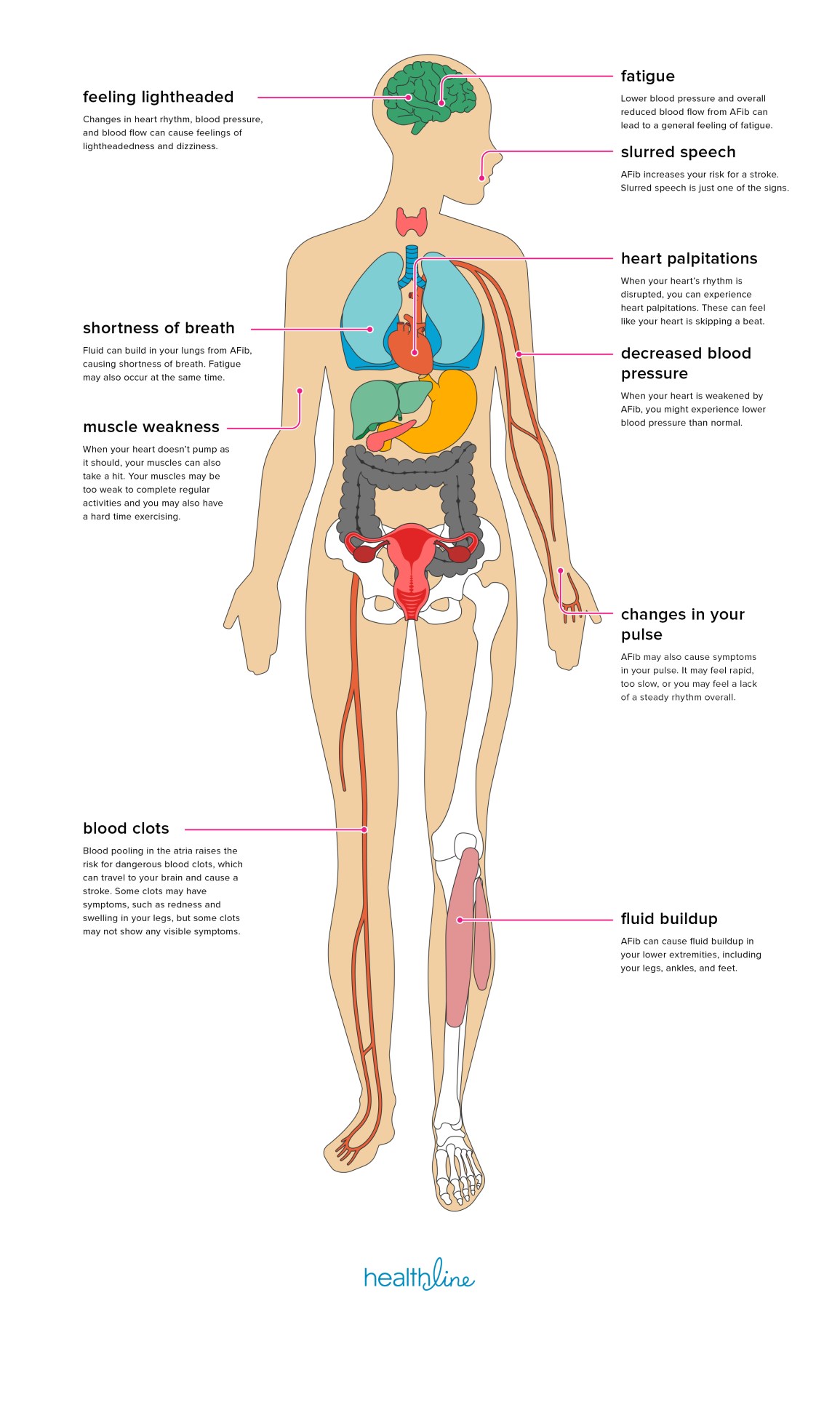
Picture this: you're already short of breath after climbing a flight of stairs, but now you feel a lingering fatigue that no amount of rest seems to shake off. That's a red flag. Other telltale clues include pallor, worsening orthopnea (that need to prop yourself up with extra pillows), and a noticeable dip in exercise tolerance. Swelling and fluid retention, also known medically as heart failure edema, can appear alongside these symptoms, making diagnosis and management more complex.
Lab Values to Watch
| Parameter | Typical Threshold | What It Means |
|---|---|---|
| Hemoglobin | <12g/dL (women) / <13g/dL (men) | Confirms anemia; triggers iron workup |
| Hematocrit | <36% (women) / <39% (men) | Reflects degree of anemia & volume status |
| Ferritin | <100ng/mL | Suggests iron deficiency |
| Transferrin Saturation (TSAT) | <20% | Another iron-deficiency marker |
Why is hemoglobin and hematocrit low in heart failure? The answer circles back to the mechanisms aboveless production, more sequestration, and sometimes outright loss.
Impact on Outcomes
How Does Anemia Change Heart Failure Prognosis?
Here's the hard truth: anemia nudges the odds of hospitalization up by roughly 80% and can nearly double short-term mortality. In a pooled analysis of over 12,000 newly diagnosed heart failure patients, those with anemia faced a 1.8-fold higher risk of any heart failure event and a 1.9-fold increase in 30-day death rates.
Prognostic Table
| Anemia Severity | 1-Year Mortality | Average Hospital Stay |
|---|---|---|
| None | 12% | 4 days |
| Mild (Hb 10-12g/dL) | 19% | 6 days |
| Moderate-Severe (Hb<10g/dL) | 28% | 9 days |
These numbers can feel intimidating, but they also point us toward where we can intervene.
Treatment Options
What Is the Best Treatment of Anemic Heart Failure?
Think of treatment as a three-step dance: first, figure out why the anemia exists; second, give the body the building blocks it needs; third, reserve blood transfusion for emergencies. Intravenous iron, particularly ferric carboxymaltose, has the strongest backingtrials like FAIR-HF2 showed a 30% drop in heart-failure hospitalizations after a single IV dose. Managing fluid overload and related swelling is equally crucial, and current edema treatment options include diuretics, compression stockings, and targeted heart failure therapy.
When Is Blood Transfusion Needed?
Transfusion isn't a first-line choice because every extra ounce of fluid can tip a fragile heart into congestion. It's generally reserved for hemoglobin <7g/dL, symptomatic instability, or when a heart attack looms. Even then, clinicians pair transfusion with diuretics and close monitoring.
Guideline Snapshot
According to the , IV iron receives a Class IIa recommendation for symptomatic patients with ferritin<100ng/mL or TSAT<20%. The European Society of Cardiology's 2022 update echoes this, urging clinicians to treat anemia only after optimizing standard heart-failure therapy.
Management Checklist
How to Diagnose and Treat Step by Step
- Screen all heart-failure patients. CBC, ferritin, and TSAT are cheap, quick, and often overlooked.
- Confirm anemia. Use the hemoglobin thresholds above.
- Pinpoint the cause. Check iron studies, kidney function, and look for sources of bleeding.
- Treat accordingly.
- Iron deficiency IV iron (per guidelines).
- Chronic disease-related anemia consider ESA only in select cases.
- Severe anemia low-volume transfusion with tight fluid balance.
- Follow-up. Recheck labs in 46 weeks, track symptoms, adjust diuretics as needed.
Self-Care Tips for You
- Keep a simple symptom diary: note fatigue levels, breathlessness, weight changes.
- Weigh yourself daily; alert your doctor if you gain more than 2lb in 24 hours.
- Boost iron intake with red meat, beans, and vitamin C-rich foods to help absorption.
Real-World Cases
Case #1: The Iron Boost
John, a 68-year-old with NYHA class III heart failure, presented with a hemoglobin of 9.2g/dL and classic fatigue. After ruling out GI bleed, he received a single dose of IV ferric carboxymaltose. Three months later, his six-minute walk distance increased by 45 meters, and he avoided any hospital admission.
Case #2: Careful Transfusion
Maria, 74, had chronic kidney disease stage 3 and a hemoglobin of 7.5g/dL after a recent bleed. The team gave her one unit of packed red cells while simultaneously administering a loop diuretic. She stabilized quickly, was discharged after two days, and her heart failure symptoms improved without fluid overload.
Both stories underline a key point: personalized carewhether it's iron or transfusioncan shift outcomes dramatically.
Bottom Line
Anemia isn't just a side note in the heart failure story; it's a major character that can rewrite the ending if we ignore it. By spotting the signs early, understanding why the heart and blood don't get along, and applying evidence-based treatments like IV iron (or judicious transfusion), we can lower hospital readmissions, boost quality of life, and maybe even add a few more years to the clock.
What's your experience with anemia and heart failure? Have you tried iron therapy, or faced a transfusion decision? Share your story in the commentsyour insights could help someone else feel less alone. And if you want a printable version of the management checklist, . Together, we can turn uncertainty into confidence and keep moving forward, one informed step at a time.
FAQs
How common is anemia among patients with chronic heart failure?
Approximately one‑third of individuals with chronic heart failure develop anemia, and prevalence rises as the disease progresses.
Which laboratory tests are essential for detecting anemia in heart‑failure patients?
Key tests include a complete blood count (hemoglobin and hematocrit), ferritin, and transferrin saturation (TSAT) to evaluate iron status.
Does intravenous iron therapy improve outcomes for heart‑failure patients with anemia?
Yes. Clinical trials such as FAIR‑HF2 have shown that a single IV dose of ferric carboxymaltose can reduce heart‑failure hospitalizations by about 30 % and improve functional capacity.
When should a blood transfusion be considered for anemic heart‑failure patients?
Transfusion is generally reserved for hemoglobin < 7 g/dL, hemodynamic instability, or acute coronary syndrome, and should be given with careful fluid management.
What can patients do at home to monitor for worsening anemia?
Keep a symptom diary (fatigue, breathlessness, orthopnea), weigh daily (alert a doctor for >2 lb gain in 24 hours), and ensure adequate dietary iron and vitamin C intake.