Below you'll find the straighttothepoint answers you're looking for: AML can involve the central nervous system, diagnosis relies on imaging and spinalfluid testing, and treatment usually mixes intrathecal chemotherapy, radiation, and newer drugs that cross the bloodbrain barrier. Lets walk through what that means for you, step by step, with a friendly, nofluff approach.
Quick Answer Overview
Can AML spread to the brain? Yes, but it happens in roughly 14% of adult cases, most often after a relapse.
How do doctors find it? MRI or CT scans plus a lumbar puncture to examine cerebrospinal fluid (CSF) are the gold standard.
What are the treatment options? Intrathecal chemotherapy, targeted radiation, and systemic agents that can cross the bloodbrain barrier (BBB) are combined to give the best chance of remission.
Now that you have the headline answers, let's dig a little deeper and explore the details you'll need when you talk to your oncologist.
Understanding AML CNS
What does central nervous system involvement really mean?
When we talk about AMLCNS involvement, we're referring to leukemia cells that have made their way into the brain, spinal cord, or the fluid that cushions them (the CSF). It's not a separate disease; it's AML that's taken a detour into a region the body tries very hard to protect.
How is AML brain metastasis different from other leukemic brain lesions?
Leukemia can cause several types of brain problems: leukoencephalopathy (a diffuse, often reversible change), bleeding from low platelets, or actual solid tumorlike lesions that look like metastases on imaging. AML brain metastasis specifically refers to clusters of leukemic blasts infiltrating the brain tissue or meninges, which often require more aggressive, targeted therapy.
Expert Insight
Dr. Sarah Miller, a hematologyoncology professor at Memorial SloanKettering, explains that CNS infiltration usually reflects aggressive disease biology, such as highrisk cytogenetics or prior highdose cytarabine exposure. Early detection can dramatically shift treatment planning. ().
Incidence and Risk
How common is AML spreading to the brain?
Large registry analyses show an incidence of around 1.1% at initial diagnosis, climbing to 2.64.1% after relapse. The risk is higher in children, but adult patients with certain highrisk genetic mutations (e.g., FLT3ITD) also face a greater chance of CNS disease.
Who is most at risk?
- Patients with relapsed or refractory AML
- Those who have received intensive cytarabine regimens
- Individuals with highrisk cytogenetics (FLT3ITD, NPM1, inv(16))
- Younger patients (especially under 30) who often receive more aggressive chemotherapy
Incidence Table
| Group | Incidence at Diagnosis | Incidence at Relapse | Typical Age |
|---|---|---|---|
| Adult AML (overall) | ~1% | ~3% | 4570 |
| Pediatric AML | ~2% | ~57% | 118 |
| Highrisk cytogenetics | ~3% | ~810% | Varies |
Spotting Early Symptoms
What neurological signs should raise a red flag?
Anything new and unexplained in the brain deserves attention. Common symptoms include:
- Persistent or worsening headaches
- Seizures (especially if you've never had one before)
- Sudden vision changes or double vision
- Confusion, memory lapses, or brain fog that feels worse than usual fatigue
- Weakness or numbness in a limb
AML encephalopathy vs. other causes of brain fog
AML encephalopathy often comes with systemic signs high fever, low blood counts, or a recent chemotherapy cycle. It's usually reversible with supportive care, whereas true CNS infiltration tends to produce focal deficits (like onesided weakness) and may not improve without specific therapy.
When to suspect a CNS relapse
If you're already in remission and suddenly develop any of the above symptoms, especially after a recent clean bonemarrow test, bring it up with your hematologist. A quick CSF analysis can catch a relapse before it spreads further.
RealWorld Example
John, a 58yearold who had been in remission for eight months, noticed a new buzzing sensation behind his eyes. He mentioned it during a routine visit; his doctor ordered an MRI, which revealed a small enhancing lesion in the left temporal lobe. A lumbar puncture confirmed AML blasts in the CSF. Early detection allowed him to start intrathecal therapy right away, extending his remission by another six months.
Diagnosis Process Explained
Which imaging modality is best?
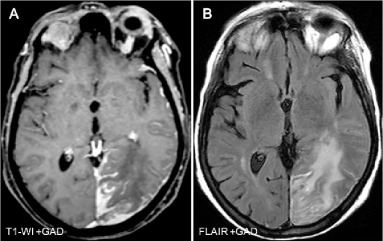
MRI with gadolinium contrast is the gold standard. It shows meningeal enhancement, parenchymal lesions, and can differentiate leukemia infiltrates from other causes like infections or hemorrhage. CT scans are used when MRI isn't feasible (e.g., pacemaker patients) but are less sensitive.
What does CSF analysis reveal?
After a lumbar puncture, the fluid is examined under a microscope (cytology) and processed with flow cytometry. Flow cytometry can detect even a few leukemic cells among hundreds of normal cells, making it the most reliable method for confirming AML CNS involvement.
Can PETCT help?
Positron emission tomography can locate occult disease in places MRI misses, especially when the disease is scattered or when you need wholebody staging. However, it's not routinely used due to cost and radiation exposure.
Diagnostic Algorithm
- Step 1: New neurological symptom Order brain MRI with contrast.
- Step 2: MRI suggests CNS disease Perform lumbar puncture.
- Step 3: CSF cytology + flow cytometry Positive Confirm AMLCNS involvement.
- Step 4: Consider PETCT for systemic disease mapping if needed.
Treatment Options Overview
What does intrathecal chemotherapy involve?
Drugs are injected directly into the CSF, bypassing the BBB. The most common regimen includes cytarabine, methotrexate, and a steroid (dexamethasone). Treatment cycles are usually given twice weekly for the first two weeks, then weekly or biweekly, depending on response.
When is radiation therapy used?
Wholebrain radiation (WBRT) or focal cranial irradiation is considered when there are bulky lesions, refractory disease after intrathecal therapy, or when rapid symptom control is needed. Typical doses range from 1218 Gy for WBRT, delivered in 69 fractions.
Which systemic drugs can cross the BBB?
Newer targeted agents like FLT3 inhibitors (midostaurin, gilteritinib) and BCL2 inhibitors (venetoclax) have shown modest CNS penetration. Clinical trials are ongoing, and enrollment can be an option for eligible patients.
For patients balancing treatment risks and quality of life, information about related cancers and treatments can be helpful for example, resources that discuss broader cancer outcomes or outlooks. You may also find discussions of surgical outcomes and life expectancy in prostate cancer useful for understanding how prognosis discussions are framed; see a concise guide on prostate cancer outlook for an example of how clinicians present survival and qualityoflife tradeoffs.
Are clinical trials worth it?
Absolutely. Trials provide access to cuttingedge therapies and often include comprehensive monitoring. Websites such as list ongoing AMLCNS studies.
Treatment Comparison Table
| Modality | Mechanism | Efficacy (CR rate) | Common SideEffects |
|---|---|---|---|
| Intrathecal Chemo | Direct drug delivery to CSF | ~55% | Headache, nausea, neurotoxicity (rare) |
| WholeBrain Radiation | DNA damage to proliferating cells | ~45% | Fatigue, alopecia, neurocognitive decline |
| Targeted Systemic (e.g., Gilteritinib) | Inhibits FLT3 signaling | ~30% (CNSspecific data limited) | Elevated liver enzymes, QT prolongation |
Prognosis and Survival
What does the prognosis look like?
Historically, AMLCNS involvement carried a poor outlook, with median overall survival (OS) of 36 months. Recent series that employ combined intrathecal chemo plus radiation report a median OS of 912 months, especially when treatment starts early.
How does survival differ between newly diagnosed and relapsed cases?
Patients diagnosed with CNS disease at initial presentation tend to have a slightly better prognosis (median OS ~11 months) compared to those who develop a CNS relapse (median OS ~46 months). The difference is largely due to disease biology and prior therapy exposure.
What factors improve outcomes?
- Early detection via MRI/CSF testing
- Prompt initiation of intrathecal therapy
- Inclusion of radiation for bulky lesions
- Eligibility for targetedtherapy trials
Survival Graphic Idea
Consider a KaplanMeier curve that separates three groups: (1) Diagnosisstage CNS disease, (2) Relapsestage CNS disease, and (3) No CNS involvement. This visual helps patients see the impact of early intervention.
Benefits vs Risks
What are the potential benefits of aggressive CNS treatment?
Therapies can shrink or eradicate brain lesions, relieve neurological symptoms, and most importantly, extend remission duration. Some patients even regain full neurologic function, allowing them to return to daily activities.
What are the main risks?
Intrathecal chemo can cause chemical meningitis, headaches, or, rarely, neurotoxicity. Radiation carries a risk of longterm cognitive decline, especially in older adults. Systemic agents may bring the usual sideeffects of chemotherapy, plus unique toxicities related to BBB penetration.
How to make a balanced decision?
Feel free to ask your oncologist for a benefitrisk matrix. Write down your personal priorities quality of life, time with family, longterm sideeffects and compare them against the expected outcomes. Shared decisionmaking is key.
Patient Stories Insight
One survivor's journey
Maria, a 42yearold mother of two, was in remission for a year when she started having blurry patches in her vision. An MRI showed a small occipital lesion, and CSF confirmed AML cells. She underwent four weeks of intrathecal cytarabine, followed by a focused radiation boost. Six months later, she's back at her kids' soccer games, with clear vision and a renewed sense of hope.
What should you ask your doctor?
- What are the chances we'll need radiation versus just chemo?
- Are there clinical trials that match my genetic profile?
- How will treatment affect my daily life and work?
Resources for Support
- HealthTree Foundation patient mentorship programs
- Leukemia & Lymphoma Society financial assistance guides
- American Cancer Society reliable information on CNS involvement
Staying Informed & Acting
How can you keep on top of CNS monitoring?
Ask your hematology team to schedule routine brain MRI scans every 36 months if you have highrisk features. A symptom diary even a simple notebook can help you track subtle changes that might otherwise be dismissed.
What steps should you take right now?
- Schedule a followup appointment to discuss any new neurological symptoms.
- Request a referral for neuroimaging if you haven't had one recently.
- Explore clinical trial options if you're open to experimental therapies.
- Connect with a support group talking to someone who's been through it can make a world of difference.
Remember, knowledge is power, and early action can tilt the odds in your favor.
Conclusion
AML brain metastasis is a rare but serious complication that demands prompt recognition and aggressive, multidisciplinary treatment. By understanding the signs, getting the right diagnostic workup, and weighing the benefits against the risks of therapy, you can make informed choices that improve both survival and quality of life. If you or a loved one faces this challenge, don't hesitate to ask your doctor about CNS screening, treatment options, and clinical trials. Stay proactive, lean on trusted resources, and keep the conversation open your health journey is a partnership, and you deserve every ounce of support.
FAQs
Can AML spread to the brain?
Yes, acute myeloid leukemia can spread to the brain, but this occurs in about 1-4% of adult AML cases, often after relapse.
How is AML brain metastasis diagnosed?
Diagnosis mainly involves MRI with contrast to detect brain lesions and a lumbar puncture to analyze cerebrospinal fluid for leukemic cells.
What treatment options are available for AML brain metastasis?
Treatment typically includes intrathecal chemotherapy, targeted radiation therapy, and systemic drugs that can cross the blood-brain barrier.
What symptoms suggest AML involvement in the brain?
Symptoms may include persistent headaches, seizures, vision changes, confusion, memory problems, weakness, or numbness.
What is the prognosis for patients with AML brain metastasis?
Prognosis is generally poor but has improved with early detection and combined therapies; median survival ranges from 9 to 12 months with prompt treatment.