Quick Answer
If youve just heard the term follicular thyroid cancer, youre probably wondering what it actually means, how you might know if you have it, and what can be done about it. In a nutshell: its a type of thyroid cancer that starts in the follicular cells of the gland, often shows up as a painless neck lump, and is usually treated with surgery followed by radioactive iodine. Most people diagnosed early enjoy excellent longterm survival.
Understanding
What Sets This Cancer Apart?
Follicular thyroid cancer (FTC) arises from the follicular cells that produce thyroid hormones. Unlike the more common papillary thyroid cancer, FTC tends to spread through blood vessels rather than lymph nodes. It accounts for roughly 1015% of all thyroid cancers, which makes it less common but still a significant health concern.
Follicular vs. Papillary
| Feature | Follicular | Papillary |
|---|---|---|
| Typical spread | Vascular (blood) | Lymphatic (nodes) |
| Common age | 4560years | 3040years |
| Prognosis (early stage) | 9095% 10yr survival | 9599% 10yr survival |
Symptoms
What Might You Notice First?
The most common warning sign is a smooth, painless nodule in the front of the neck. Some people also feel a mild pressure when swallowing or notice a subtle change in voice. Because these clues can be so easy to overlook, its worth paying extra attention if you feel somethings not quite right in that area.
When Symptoms Suggest Spread
If the tumor has begun to spread (what doctors call FTC spread), you may develop hoarseness, persistent cough, or even shortness of breath. These symptoms happen when the cancer reaches nearby structures or travels to the lungs. If any of these appear suddenly, its a good idea to get checked right away.
Symptom Checklist
- New lump or swelling in neck
- Difficulty swallowing or a feeling of tightness
- Persistent hoarseness or voice change
- Unexplained weight loss or fatigue
- Cough that wont go away
Causes & Risks
Why Does FTC Happen?
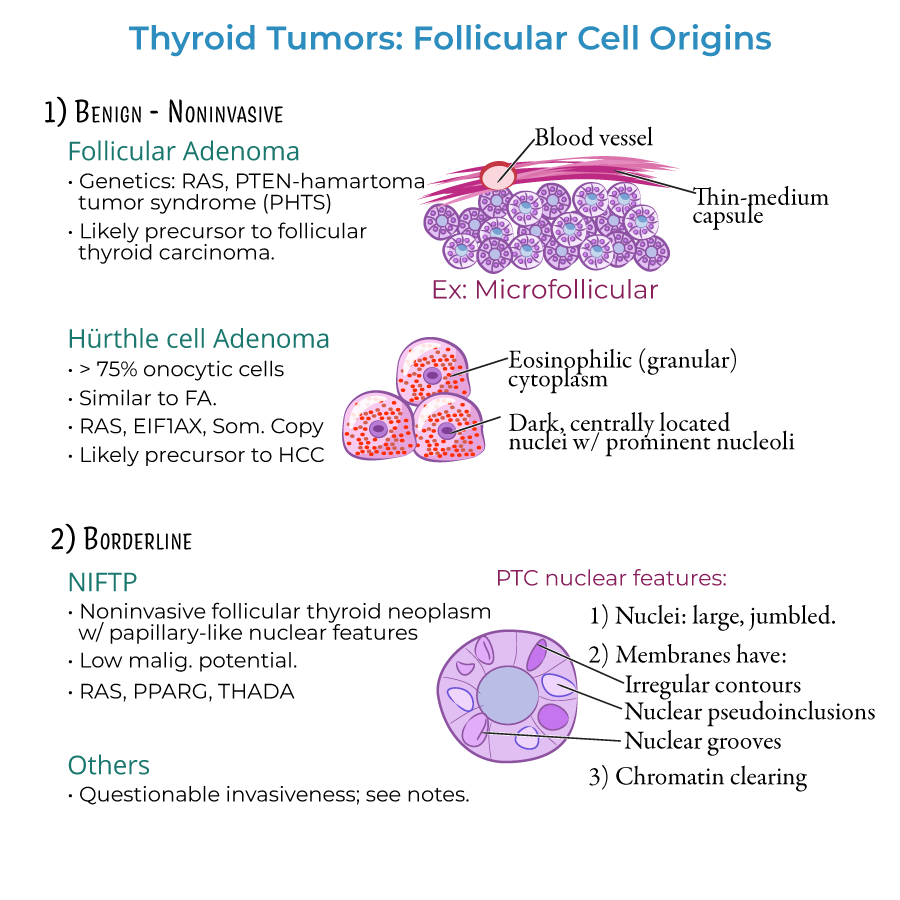
Theres no single cause that explains every case, but several risk factors tip the odds. Prior exposure to radiation (especially during childhood), a diet low in iodine, and being a woman over 50 all increase the chance of developing FTC. On the genetic side, mutations in the RAS gene or the PAX8PPAR fusion are frequently seen in tumor tissue.
How You Can Reduce Risk
While you cant change your genetics, maintaining adequate iodine intake and avoiding unnecessary radiation exposure are practical steps. If you lived through a nuclear incident or had head/neck radiation as a child, its worth discussing thyroid monitoring with your doctor.
RiskFactor Wheel (Idea)
Imagine a colorful wheel where each slice represents a risk factorage, gender, radiation, iodine, genetics. Visualizing it can help you see how multiple small factors add up.
Diagnosis & Staging
How Doctors Confirm FTC
The workup starts with a physical exam and a highresolution neck ultrasound. If a nodule looks suspicious, the next step is a fineneedle aspiration (FNA) biopsy. The pathology lab then looks for capsular or vascular invasionkey hallmarks of FTC that differentiate it from benign nodules.
Pathology & Histology
On the microscope slide, follicular cells line small, uniform follicles. The decisive clue is whether the tumor has broken through the capsule (capsular invasion) or entered blood vessels (vascular invasion). These findings are detailed in most .
Staging the Disease
The American Joint Committee on Cancer (AJCC) TNM system is used worldwide. StageI and II mean the tumor is confined to the thyroid, while StageIIIIV indicates spread to nearby lymph nodes, lungs, or bones. Staging helps predict the and guides treatment decisions.
Stage Overview
| Stage | Criteria | Typical 10yr Survival |
|---|---|---|
| I | Any tumor 2cm, no spread | 98% |
| II | Tumor>2cm but 4cm, no spread | 95% |
| III | Any size with limited regional spread | 85% |
| IV | Distant metastasis (lungs, bone) | 60% |
Treatment Options
FirstLine: Surgery
For most patients, the cornerstone of treatment is surgeryeither a total thyroidectomy (removing the entire gland) or a lobectomy (removing just the affected lobe). The choice depends on tumor size, location, and whether theres evidence of spread.
Radioactive Iodine (RAI) Therapy
After surgery, many doctors recommend radioactive iodine ablation. Since thyroid cells naturally take up iodine, a high dose of I131 can hunt down any remaining cancer cells without harming other tissues. RAI is especially helpful when the tumor shows vascular invasion.
Other Treatments
- External Beam Radiation: Reserved for unresectable or locally advanced disease.
- Targeted Therapies: Multikinase inhibitors (e.g., sorafenib, lenvatinib) are options for progressive metastatic FTC.
- Thyroid Hormone Replacement: Lifelong levothyroxine keeps your metabolism stable and suppresses TSH, which can stimulate cancer growth.
Surgery vs. RAI vs. Systemic Therapy
| Option | Goal | Pros | Cons |
|---|---|---|---|
| Surgery | Remove visible tumor | High cure rate for localized disease | Risk of voice changes, calcium loss |
| RAI | Destroy residual cells | Noninvasive, targets hidden disease | Dry mouth, temporary taste changes |
| Targeted drugs | Control metastatic spread | Effective when other therapies fail | Side effects (high blood pressure, skin issues) |
Prognosis & Survival
What the Numbers Say
Overall, FTC has a favorable outlook when caught early. The follicular thyroid cancer survival rate for stageIII disease exceeds 90% at ten years. Even for stageIII, many patients live much longer than the statistics suggest, thanks to advances in RAI and targeted therapies.
Factors That Influence Outlook
Age at diagnosis, tumor size, and whether vascular invasion is present are the biggest predictors. Younger patients (<45years) generally fare better, and complete surgical removal combined with appropriate RAI dramatically improves chances of staying diseasefree.
Survival Curve (Illustrative)
Picture a gently rising line for stageI that flattens near the top (98%). As you move to stageIV, the line drops steeper, but even then many patients survive beyond five years with modern treatments.
When to Seek Help
RedFlag Scenarios
Not all neck lumps are cancer, but you shouldnt ignore them. Call your doctor promptly if you notice any of these:
- Rapid growth of a neck mass
- Sudden hoarseness or voice loss
- Difficulty breathing or swallowing
- Persistent cough not linked to a cold
Early evaluation can mean the difference between a simple surgery and more extensive treatment.
Final Thoughts
Follicular thyroid cancer can feel scary at first glance, but the good news is that its often treatable, especially when caught early. By staying alert to subtle symptoms, understanding the risk factors, and working closely with a knowledgeable endocrinologist or thyroid surgeon, you can navigate the journey with confidence. Remember, youre not alonetheres a whole community of patients, doctors, and researchers dedicated to improving outcomes.
If you have questions or want to share your own experience, feel free to reach out to a qualified thyroid specialist. Knowledge, support, and early action are the best tools we have. For related information on treatment outcomes and long-term outlook after major cancer surgeries, see prostate cancer outlook.