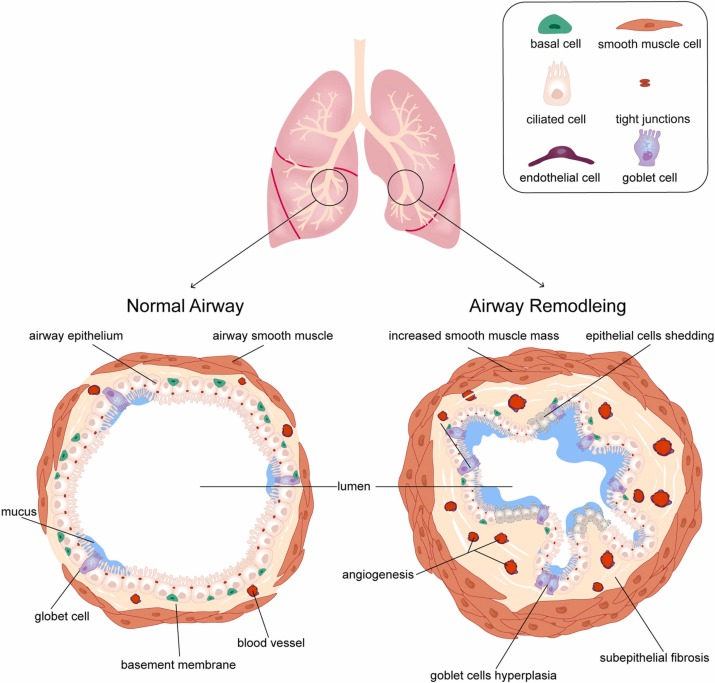
Imagine your airways are a smooth garden hoseflexible, easy to bend, and ready to deliver a strong stream of air whenever you need it. Now picture that hose slowly gaining thick, stiff layers of wax, making it harder to turn the water on. Thats essentially what airway remodeling in asthma looks like: the walls of your bronchi thicken and scar, turning a reversible airway problem into a more permanent obstacle.
In the next few minutes well cut through the medical jargon, share realworld stories, and give you a clear roadmap for spotting the signs, understanding the causes, and taking action. Whether youre living with asthma yourself, caring for someone who is, or just curious, youll walk away with practical steps you can use today.
What Is Remodeling
Definition & Core Features
When doctors talk about airway remodeling meaning, they refer to permanent structural changes in the airway wall. These changes include:
- Thickening of the smoothmuscle layer (smoothmuscle hypertrophy)
- Increased collagen and fibrous tissue beneath the lining (subepithelial fibrosis)
- More mucusproducing goblet cells (gobletcell hyperplasia)
- Reduced elasticity, which makes the airway less able to open on demand
Think of it like a scar that gets deeper each time the skin is injured. Each asthma flare can add another layer to the airway wall.
How It Differs From Simple Inflammation
Inflammation is the bodys shortterm response to irritantslike a brief swelling that goes down with a bronchodilator. Remodeling, on the other hand, is a longterm, structural shift that doesnt fully reverse with typical rescue inhalers.
| Aspect | Inflammatory Asthma | RemodelingDominant Asthma |
|---|---|---|
| Reversibility (FEV) | 15% improvement after bronchodilator | <5% improvement |
| Imaging | Usually normal | Wall thickening, airtrapping on CT |
| Biomarkers | Eosinophils , FeNO | Fibrogrowth factors , collagen markers |
Why It Happens
What Causes Airway Remodeling in Asthma
Several forces work together, a bit like the combination of heat, moisture, and pressure that slowly bends a metal rod:
- Chronic inflammation cytokines such as IL4, IL5, and TGF drive tissue remodeling.
- Repeated exacerbations each flare adds a new layer of scar tissue.
- Genetic predisposition certain gene variants (e.g., filaggrin) make the airway lining more vulnerable.
- Environmental irritants tobacco smoke, occupational dust, and even viral infections can accelerate the process.
In short, what causes airway remodeling in asthma is a perfect storm of ongoing inflammation, exposure, and individual biology.
RealWorld Example
Take Mark, a 37yearold graphic designer who thought his bad asthma was just part of his personality. He smoked a few cigarettes on weekends and stopped his inhaled corticosteroid whenever he felt okay. After three years of frequent nighttime wheeze and an increasing need for rescue inhaler, a highresolution CT revealed noticeable wall thickening. Marks story illustrates how everyday habits and missed medication can tip the balance toward permanent change.
Spotting Symptoms
Airway Remodeling Symptoms
If youre wondering airway remodeling symptoms, look for signs that differ from a typical asthma flare:
- Persistent cough that doesnt improve with a shortacting bronchodilator
- Reduced response to inhaled steroids (you feel the same even after using them correctly)
- Nighttime breathlessness that wakes you up more than once a week
- Gradual decline in peak flow readings over months, not just during attacks
These clues signal that the airway walls may be stiffening. A simple lung function test (spirometry) often shows a fixed reduction in the FEV/FVC ratio.
Diagnostic Toolbox
Doctors combine a few tools to confirm remodeling:
- HighResolution CT (HRCT) graphic images that reveal wall thickness.
- Impulse Oscillometry measures airway resistance in real time, helping spot fixed obstruction.
- Spirometry the classic test that shows a limited reversibility after bronchodilator use.
Can It Reverse
Is Airway Remodeling Reversible?
Great questionone that many patients ask. The short answer is: its partially reversible if caught early. A 2023 systematic review published in found that biologic agents targeting IL5, IL4R, or TSLP produced modest reductions in airway wall thickness when started within the first five years of asthma diagnosis.
Factors that Influence Reversibility
- Early detection the sooner the wall thickening is identified, the more likely treatment can halt further scarring.
- Adherence to controller therapy daily inhaled corticosteroids (ICS) remain the cornerstone.
- Asthma phenotype eosinophilic (type2) inflammation tends to respond better to biologics than neutrophilic patterns.
Quick Checklist for You
Ask yourself these questions:
- Have I had asthma for less than five years?
- Do I use my inhaled corticosteroid every day, as prescribed?
- Have I experienced two or more severe exacerbations in the past year?
- Would I be a candidate for a biologic therapy after a specialists assessment?
If you answered yes to most of these, you have a good chance of slowingor even slightly reversingremodeling.
Treatment Options
Airway Remodeling Treatment Overview
When it comes to airway remodeling treatment, the goal is twofold: reduce ongoing inflammation and remodel the structure itself where possible.
Pharmacologic Strategies
- Inhaled Corticosteroids (ICS) the first line; highdose options can curb the cytokine cascade that fuels scarring.
- Biologic Therapies antiIL5 (e.g., mepolizumab), antiIL4R (dupilumab), and antiTSLP (tezepelumab) have all shown benefit in reducing wall thickness in clinical trials.
- Bronchial Thermoplasty a onetime bronchoscopy that heats airway smoothmuscle to reduce its mass. Its a niche option for severe, refractory cases.
NonPharmacologic Approaches
Dont underestimate the power of everyday choices:
- Quit Smoking even secondhand exposure can accelerate remodeling.
- Control Occupational Exposures wear masks or improve ventilation if you work with dust or chemicals.
- Weight Management excess weight can increase airway inflammation.
- Pulmonary Rehabilitation breathing exercises improve airway mechanics and overall stamina.
StepbyStep Management Algorithm (Simplified)
- Confirm remodeling via HRCT or persistent fixed obstruction on spirometry.
- Optimize highdose inhaled corticosteroid/longacting betaagonist (ICS/LABA) therapy.
- Evaluate eligibility for a biologic (consult allergist or pulmonologist).
- Consider bronchial thermoplasty if severe disease persists despite maximal medical therapy.
- Implement lifestyle modifications and regular followup.
Other Lung Diseases
Airway Remodeling in COPD
While asthma gets most of the spotlight, airway remodeling in COPD shares many featuresfibrosis, smoothmuscle hypertrophy, and reduced reversibility. However, the driving cytokine milieu differs (more neutrophilic inflammation, less eosinophilic). Understanding the overlap helps clinicians decide if a patient truly has asthmaCOPD overlap and tailor therapy accordingly.
Impact on Life Expectancy
Longterm studies suggest that fixed airflow limitation can modestly affect airway remodeling life expectancy. Patients with severe, untreated remodeling may experience a slightly higher risk of cardiovascular complications due to chronic hypoxia. The good news? Early, aggressive treatment improves survival rates comparable to those without remodeling.
RealWorld Stories
Patient Voice
I thought my asthma was just bad until a CT showed thickened walls. Switching to an IL5 blocker cut my rescue inhaler use from three times a day to once a week. It felt like I got my life back, says Sarah, a 42yearold teacher. Her journey highlights how targeted therapy can change the narrative from hopelessness to control.
Clinician Insight
Dr. Lina Patel, a boardcertified pulmonologist, explains, We no longer wait for a lifethreatening crisis to investigate remodeling. Early CT and biomarker assessment let us intervene with biologics before the airway wall becomes a permanent scar. Her advice to patients echoes the articles core message: proactive care beats reactive panic.
Putting It All Together
Understanding airway remodeling in asthma is like learning to read the subtle signs of a road trip youve been on for years. The path may get bumpy, but with the right mapearly detection, consistent medication, and perhaps a biologic boostyou can keep the journey smooth.
Remember, youre not alone in this. Talk to your doctor about a highresolution CT if youve had repeated exacerbations or notice a decline in lung function. Ask whether you qualify for newer therapies, and never underestimate lifestyle tweaks like quitting smoking or staying active.
Whats one step you feel ready to take today? Whether its scheduling that appointment, setting a reminder to use your inhaler, or simply learning more about biologic options, each small move brings you closer to breathing easier. Also consider practical support for people with long-term respiratory conditionsrelationships and daily safety matter, so resources on cystic fibrosis safety can offer useful tips that overlap with airway care.
FAQs
What is airway remodeling in asthma?
Airway remodeling in asthma refers to permanent structural changes in the airway walls, such as smooth muscle thickening, subepithelial fibrosis, goblet cell increase, and reduced airway elasticity, leading to persistent airway obstruction.
How does airway remodeling differ from asthma inflammation?
Inflammation is a short-term response causing reversible airway swelling and obstruction that improves with bronchodilators, while remodeling represents long-term, often irreversible structural changes that do not fully respond to typical asthma medications.
Can airway remodeling in asthma be reversed?
Airway remodeling is partially reversible if detected early, especially within five years of diagnosis. Treatments like inhaled corticosteroids and biologic agents targeting IL5, IL4R, or TSLP can reduce airway wall thickening and slow progression.
What are common signs that airway remodeling may be occurring?
Signs include a persistent cough unresponsive to bronchodilators, reduced response to inhaled steroids, frequent nighttime breathlessness, and a gradual decline in lung function measurements such as the FEV/FVC ratio.
What treatment options are available for airway remodeling in asthma?
Treatment includes high-dose inhaled corticosteroids, biologic therapies (anti-IL5, anti-IL4R, anti-TSLP), bronchial thermoplasty for severe cases, and lifestyle changes like quitting smoking and managing environmental exposures.