Lets cut to the chase: immunotherapy is changing the game for many breastcancer patients, but exactly how well does it work? In a nutshell, earlystage triplenegative breast cancer (TNBC) sees a pathologic complete response (pCR) of roughly 6065% when immunotherapy is paired with chemotherapy, while metastatic disease (stage4) typically enjoys an overall response of 1525% and a modest extension of overall survival by a few months. Below, Ill walk you through the numbers, the science, the sideeffects, and the realworld considerations so you can feel confident about what these stats really mean for you or a loved one.
Why Immunotherapy Matters
Traditional chemo attacks rapidly dividing cells, but it cant tell the difference between a tumor and a healthy cell. Immunotherapy, on the other hand, wakes up your own immune system to recognize and destroy cancer cellskind of like giving a tired security guard a megaphone and a fresh cup of coffee.
Most breastcancer immunotherapies target the PD1/PDL1 checkpoint pathway. When this brake is released, Tcells can chase down cancer cells more aggressively. The biggest players right now are pembrolizumab (Keytruda) and atezolizumab (Tecentriq), both of which have earned FDA approval for specific breastcancer subtypes.
The data are clear: checkpoint inhibition is a powerful lever in triplenegative disease, says Dr. LauraMiller, a boardcertified oncologist at the Cleveland Clinic. , these agents have become a cornerstone of modern treatment protocols.
Success by Stage
| Subtype / Stage | Key Trial(s) | pCR / ORR | Median OS / 2yr Survival |
|---|---|---|---|
| TNBC Stage12 (early) | KEYNOTE522 (2022) | 64.8% pCR | |
| TNBC Stage3 (locally advanced) | IMpassion031 (2021) | 44% ORR | |
| HRpositive / HER2negative Stage12 | Earlyphase combo studies | 2030% pCR | |
| Metastatic (Stage4) PDL1positive TNBC | KEYNOTE355 (2022) | 19% ORR | 23mo OS |
| Metastatic HRpositive | Limited data | 1012% ORR |
What does a pCR mean for my prognosis?
A pathologic complete response means no invasive cancer is found in the breast or lymph nodes after surgery. Studies show that patients who achieve pCR after neoadjuvant immunotherapy + chemo have a 5year diseasefree survival rate exceeding 80%. In plain English: the odds of staying cancerfree for half a decade dramatically improve.
Factors That Influence Success
Tumor Biology
Not all breast cancers are created equal. High PDL1 expression, the presence of tumorinfiltrating lymphocytes, and a triplenegative hormone profile make a tumor more likely to respond. Hormonereceptorpositive or HER2negative cancers tend to have lower response rates, though research is ongoing.
Treatment Regimen
Immunotherapy shines brightest when combined with chemotherapy. In earlystage disease, pembrolizumab is given every three weeks alongside standard anthracyclinetaxanebased regimens. In metastatic settings, the drug may continue until disease progression or unacceptable toxicity.
PatientSpecific Variables
- Age and overall healthpatients with a strong performance status (>70 on the ECOG scale) tend to tolerate and benefit from checkpoint blockade better.
- Prior lines of therapyearlier use often yields higher response rates.
- Comorbidities such as autoimmune disease can increase the risk of immunerelated side effects.
Quick Checklist for Your Next Oncologist Visit
- Ask about your tumors PDL1 score.
- Confirm whether your cancer subtype (TNBC, HRpositive, HER2negative) matches the approved indication.
- Discuss the planned duration of immunotherapy.
- Understand the monitoring plan for potential side effects.
RealWorld Effectiveness & Limitations
What the Data Shows vs. What Happens in the Clinic
Large PhaseIII trials like KEYNOTE522 and IMpassion031 give us the headline numbers, but realworld registries report a slightly lower realworld pCR rate of about 55% (see a 2022 ). The discrepancy often stems from broader patient populationspeople with coexisting health issues who wouldnt qualify for a tightly controlled trial.
Side Effects You Should Know
Immunerelated adverse events (irAEs) are the flip side of a revvedup immune system. Commonly reported issues include:
- Skin rash or itching (15%).
- Colitis, which can cause diarrhea and abdominal pain.
- Endocrine disorders such as hypothyroidism or adrenal insufficiency.
- Liver inflammation (hepatitis).
Most grade34 toxicities can be managed with corticosteroids if caught early, so regular blood work and symptom tracking are essential.
Cost Considerations
A single year of pembrolizumab can run between $120,000 and $150,000 in the United States. Insurance coverage varies, but many pharmaceutical companies offer patientassistance programs that can offset outofpocket costs. Understanding the financial impact is part of the treatment decision, notes Dr. Miller.
CostvsBenefit Snapshot
Imagine a patient with earlystage TNBC who achieves a pCR thanks to immunotherapy. The added cost translates into an estimated 0.5to1qualityadjusted lifeyear (QALY) gain, a ratio that many healtheconomics models deem acceptable for lifeextending therapies.
How to Talk to Your Oncologist
Preparation is power. Bring a copy of your pathology report, ask for the exact PDL1 percentage, and write down any questions you have. Heres a sample script you can adapt:
I read that pembrolizumab added to chemotherapy can increase the pathologic complete response in earlystage triplenegative breast cancer. Based on my tumors PDL1 level and overall health, do you think Im a good candidate, and what should I expect in terms of benefits and side effects?
Dont be shy about asking about clinical trials eitheroften they provide access to cuttingedge combinations that may improve outcomes further.
Bottom Line and Next Steps
Immunotherapy offers a real chance at better outcomes, especially for earlystage triplenegative breast cancer where pCR rates climb to the mid60% range. For metastatic disease, the gains are more modest but still meaningfuladding a few months of life and potentially improving quality of those months.
But its not a freeforall. The benefits must be weighed against the possibility of immunerelated side effects, the financial burden, and the specific biology of each tumor. The best way to navigate this landscape is an open, honest conversation with a knowledgeable oncologist, armed with the right questions and a clear understanding of what the data really say.
Ready to take the next step? Download our printable Immunotherapy FAQ (link below) or sign up for updates on emerging trials. And if youve walked this path before, please share your experience in the commentswe all learn more when we talk openly.
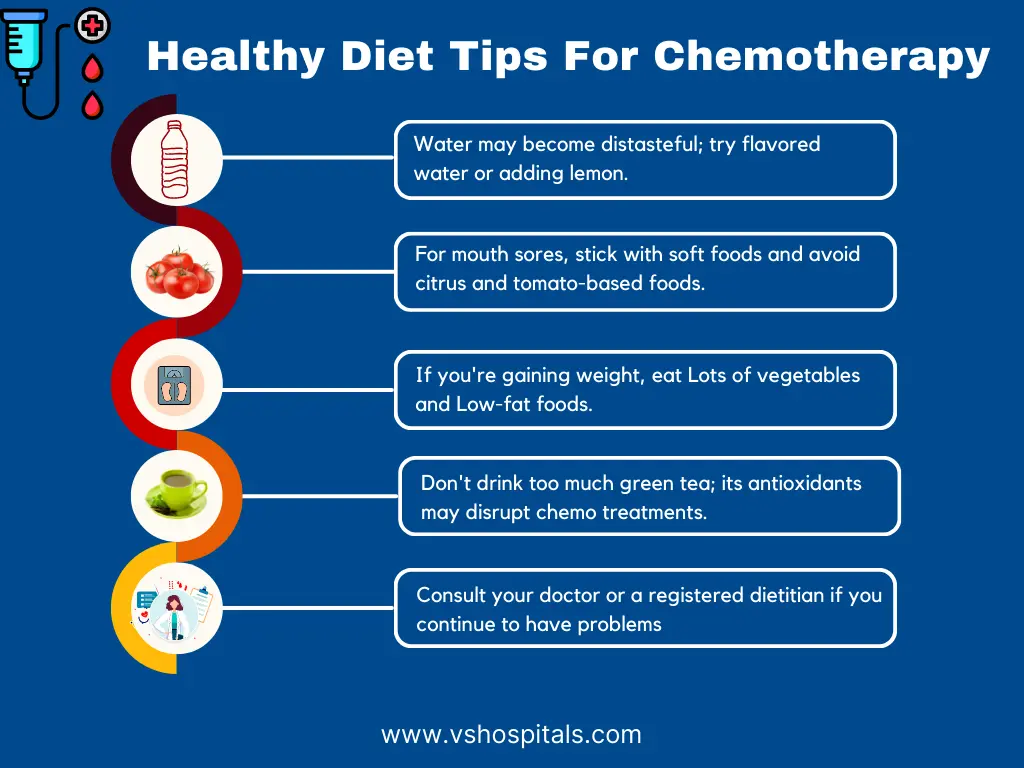
For patients concerned about broader cancer care topics like nutrition and recovery after major procedures, consider reading guidance on Cancer diet plan to help plan meals and support recovery during therapy.
FAQs
What is the overall success rate of immunotherapy for breast cancer?
The success rate varies by stage: early‑stage triple‑negative breast cancer (TNBC) achieves a pathologic complete response (pCR) in about 60‑65 % of patients, while metastatic disease shows an overall response rate of roughly 15‑25 %.
Which breast‑cancer subtypes respond best to immunotherapy?
Triple‑negative breast cancer (TNBC) with high PD‑L1 expression and abundant tumor‑infiltrating lymphocytes tends to respond most robustly. Hormone‑receptor‑positive or HER2‑negative cancers have lower response rates.
How is immunotherapy administered in the neoadjuvant (pre‑surgery) setting?
In early‑stage disease, agents such as pembrolizumab are given every three weeks together with standard anthracycline‑taxane chemotherapy, typically for a total of four to six cycles before surgery.
What are the most common immune‑related side effects?
Patients may experience skin rash, colitis, endocrine disorders (like hypothyroidism), and hepatitis. Most grade 3–4 toxicities can be managed with corticosteroids if identified early.
Can I combine immunotherapy with other clinical trials or treatments?
Yes—many trials are exploring combinations of checkpoint inhibitors with targeted therapies, vaccines, or novel agents. Discuss trial eligibility with your oncologist to access cutting‑edge options.