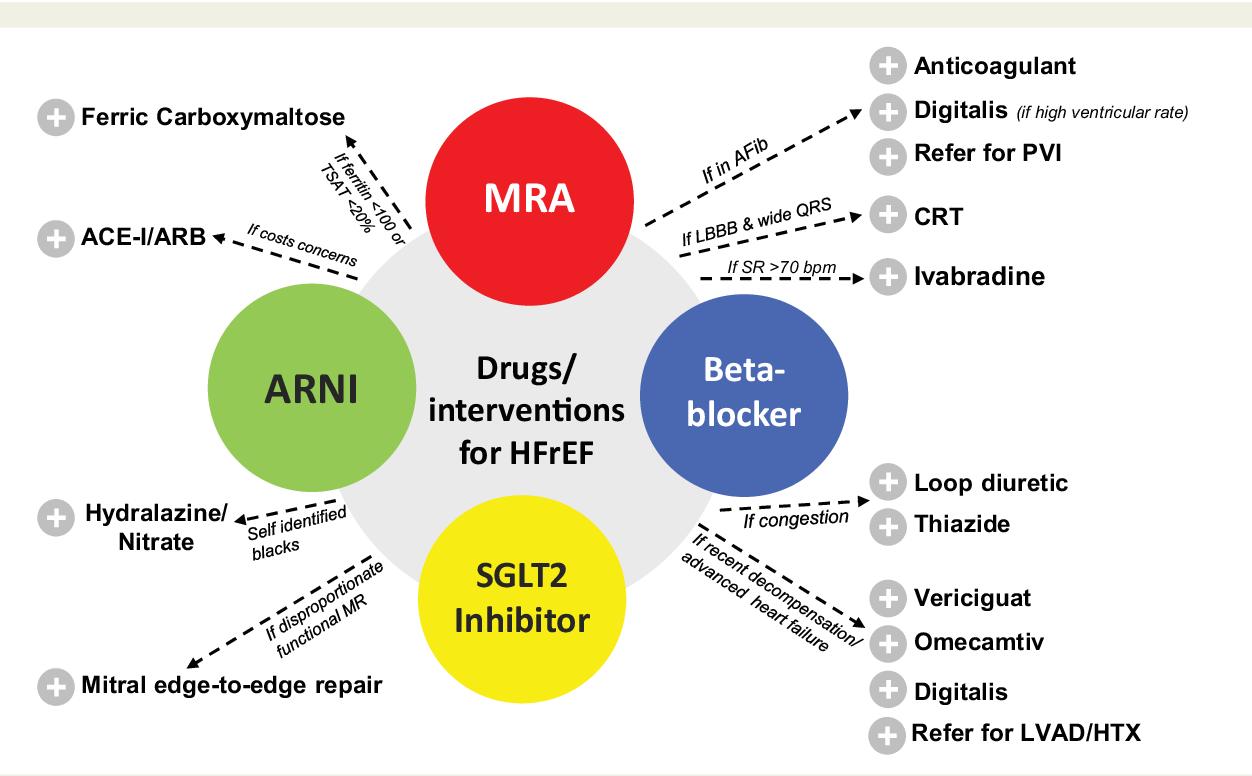
The Fantastic Four
When cardiologists talk about the fantastic four, they mean exactly these four classes. The phrase started appearing in the ESC and AHA/ACC a few years ago, and its stuck because its both catchy and accurate. Think of it as the four pillars holding up a house: each one supports the structure, but you need all of them for the roof to stay solid.
What does the Fantastic Four concept mean?
In simple terms, the concept says that if a patient with reducedejectionfraction heart failure can tolerate all four, they will experience the biggest drop in mortality and the most improvement in quality of life. The guidelines recommend starting these drugs early, then carefully titrating each to the target dose that clinical trials showed works best.
When did these drugs become standard?
It wasnt an overnight shift. ACE inhibitors dominated the 1990s, then ARBs took a slice of the pie. In 2014 the PARADIGMHF trial introduced the ARNI (sacubitril/valsartan), which quickly climbed to topranked status. Betablockers have been around since the early 2000s for heart failure, while MRAs like spironolactone earned a spot after the RALES trial in 1999. The newest star, SGLT2 inhibitors, entered the heartfailure arena in 2020 with the DAPAHF and EMPERORReduced trials. Now theyre all sitting sidebyside in the guidelines.
ARNI Explained
The ARNI (AngiotensinReceptorNeprilysin Inhibitor) is the newest hero of the list. Its brand name is Entresto, a combination of sacubitril and valsartan. Think of it as a twoinone superhero: valsartan blocks the badacting angiotensin II, while sacubitril stops the breakdown of natriuretic peptides that help the heart relax.
How does an ARNI work?
When the heart is weak, it releases natriuretic peptides that tell the kidneys to get rid of excess fluid and blood vessels to widen. Neprilysin, an enzyme, usually destroys these peptides. Sacubitril says nope to neprilysin, letting the peptides stay longer. Meanwhile, valsartan shuts down the angiotensin II pathway that makes blood vessels tighten and the heart work harder.
Commonly prescribed ARNI
Most patients start on a low dose (24/26mg twice daily) and double every two weeks as tolerated, aiming for the target dose of 97/103mg twice daily. The goal is to reach the dose that showed a 20% reduction in cardiovascular death in the PARADIGMHF trial.
Who should take it?
Ideal candidates are those with an ejection fraction 40% who have no history of angioedema and whose kidneys are functioning reasonably well (eGFR>30mL/min/1.73m). If youre already on an ACE inhibitor, you need a 36hour washout before switching to an ARNI to avoid a rare but serious swelling of the airway.
Benefits & risks
- Benefits: Lower mortality, fewer hospitalizations, better symptoms, and a modest drop in blood pressure.
- Risks: Potential for low blood pressure, dizziness, kidney function changes, and, very rarely, angioedema.
Realworld tip
When I first switched a 68yearold patient from lisinopril to Entresto, he was nervous about new meds. I told him to watch for lightheadedness and to call if he felt faint. He started at a low dose, felt a little dizzy the first week, but after titrating up he reported being able to walk his dog longer without gasping. Simple, right?
BetaBlocker Basics
Betablockers are the quiet, steady backbone of the regimen. They calm the frenetic adrenaline surge that a failing heart loves to chase, giving the muscle a chance to rest and recover.
Why betablockers are essential
In heart failure, the sympathetic nervous system goes into overdrive, pumping out norepinephrine that makes the heart beat faster and harder. Over time, this wears the heart out. Betablockers blunt that signal, lowering heart rate and allowing the heart to fill more fully between beats.
Firstline agents
The three that have the strongest evidence are:
- Carvedilol (a nonselective blocker with extra antioxidant properties)
- Metoprolol succinate (ToprolXL)
- Bisoprolol
All three are on the in the latest AHA guidelines.
Dosing & titration
Start low (e.g., carvedilol 3.125mg twice daily) and double every two weeks as tolerated, aiming for carvedilol 25mg twice daily, metoprolol succinate 200mg daily, or bisoprolol 10mg daily. Keep an eye on blood pressure, heart rate (target 5060bpm), and any signs of fatigue.
Benefits & sideeffects
- Benefits: Reduces death risk by about 35%, improves exercise capacity, and lessens arrhythmias.
- Sideeffects: May cause initial fatigue, cold hands/feet, mild bronchospasm in asthma, or a slower heart rate.
Patient story
One of my patients, a retired teacher, told me he felt like a snail after the first few weeks on carvedilol. We paused, reduced the dose, and then slowly built back up. After three months he could climb two flights of stairs without stopping a huge win that made the early snail feeling worth it.
MRA Overview
Mineralocorticoid Receptor Antagonists (MRAs) act like a safety net against a sneaky hormone called aldosterone, which makes the heart retain salt and water and promotes scarring.
What classifies an MRA?
MRAs block the receptor that aldosterone binds to, preventing sodium retention and the stiffening of heart tissue. The two most common drugs are spironolactone and its more selective cousin, eplerenone.
Leading drugs
- Spironolactone (Aldactone) cheaper, but can cause mild breast tenderness or male pattern hair growth.
- Eplerenone (Inspra) less hormonal sideeffects, but a bit pricier.
Who benefits most?
Patients who have already started an ARNI and a betablocker, especially those with a history of heart attack, low ejection fraction, or persistent fluid buildup, are prime candidates. The RALES and EMPHASISHF trials proved that adding an MRA can shave off another 15% of deaths.
Risks to monitor
The big one is hyperkalemia (high potassium). Before starting, check potassium and kidney function, then repeat labs after one week, one month, and quarterly thereafter. If potassium climbs above 5.5mmol/L, dosage adjustments or a switch to eplerenone may be needed.
Practical checklist
| Step | When to Check | What to Look For |
|---|---|---|
| Baseline labs | Before starting | Potassium <5.0mmol/L, eGFR>30mL/min |
| First followup | 1week | Potassium rise? |
| Second followup | 1month | Stable kidneys? |
| Routine monitoring | Every 3months | Any new meds that raise potassium? |
SGLT2 Inhibitor
At first glance, a diabetes drug might seem out of place in a heartfailure regimen. Yet SGLT2 inhibitors have become the new wonder drug for heart failure because they do more than lower blood sugar they drain excess fluid, lower blood pressure, and improve heart metabolism.
Why a diabetes drug belongs in HF therapy
SGLT2 stands for SodiumGlucose CoTransporter2. By blocking this transporter in the kidneys, the drug causes the body to excrete glucose and water. The resulting mild diuresis reduces preload (the amount of blood returning to the heart), and the shift in heart energy use makes the myocardium more efficient.
Approved agents
- Dapagliflozin (Farxiga)
- Empagliflozin (Jardiance)
Both have FDA approval for heart failure with reduced ejection fraction regardless of diabetes status.
Indications beyond diabetes
Even patients with normal blood sugar can start an SGLT2 inhibitor if they have an EF40% and are on the other three drugs. The DAPAHF trial showed a 27% reduction in cardiovascular death or hospitalization.
Benefits & cautions
- Benefits: Fewer heartfailure admissions, lower CV mortality, modest weight loss, and bloodpressure drop.
- Cautions: Risk of genital yeast infections, mild dehydration, and rare ketoacidosis (especially in type1 diabetics).
New wonder drug mythbusting
Its tempting to call SGLT2 inhibitors a miracle, but theyre a pillar, not a replacement. They work best when added to the ARNI, betablocker, and MRA, creating a synergistic effect that tackles heart failure from four angles.
How They Work Together
Imagine your heart as a car engine. The ARNI clears the exhaust, the betablocker eases the throttle, the MRA stops the engine from rusting, and the SGLT2 inhibitor fuels it with cleaner gasoline. When all four run together, the engine runs smoother, lasts longer, and uses less fuel.
Mechanistic complementarity
- ARNI + BetaBlocker: Controls both the reninangiotensinaldosterone system (RAAS) and the sympathetic nervous system.
- MRA + SGLT2i: Handles fluid overload and metabolic stress, while also protecting the kidneys.
Clinical evidence of combined therapy
Metaanalyses of PARADIGMHF, DAPAHF, and EMPERORReduced data show that patients on all four drugs have a 35% lower risk of death compared with those on just an ACE inhibitor and a betablocker. The benefit is additive, not just overlapping.
Comparison table
| Drug Class | Primary Target | Key Benefit | Common SideEffect |
|---|---|---|---|
| ARNI | RAAS + Natriuretic peptides | mortality, hospitalisation | Low BP, dizziness |
| BetaBlocker | Sympathetic nervous system | survival, arrhythmia | Fatigue, bradycardia |
| MRA | Aldosterone receptor | fibrosis, potassium excretion | Hyperkalemia |
| SGLT2i | Kidney glucose reabsorption | HF admissions, metabolic benefit | Genital infection |
Practical Tools for You
Now that the science is clear, lets talk about what you can do today.
Firstvisit checklist
- Bring a list of current meds (including overthecounter).
- Know your recent lab numbers especially potassium and kidney function.
- Ask your doctor about a stepwise plan to add each drug, starting low and titrating slowly.
Medicationadherence apps
Apps like Medisafe or MyTherapy send reminders, track doses, and let you log sideeffects. A quick daily ping can be the difference between staying on target and missing a dose.
When to call your doctor?
- Sudden weight gain (>2kg in 3days) possible fluid retention.
- New dizziness or fainting could be low blood pressure.
- Persistent cough or wheeze after starting an ARNI or betablocker.
- Swelling or itching in the genital area after starting an SGLT2i.
Case vignette
John, 55, was diagnosed with HFrEF (EF35%). He started on carvedilol 12.5mg BID and sacubitril/valsartan 24/26mg BID. After 4weeks, his potassium was 4.8mmol/L, so we added spironolactone 12.5mg daily. Two months later, his doctor introduced dapagliflozin 10mg daily. Six months in, Johns NYHA class improved from III to II, his BNP dropped by 40%, and he hasnt been hospitalized. His story shows the power of the fourpill regimen when followed stepbystep.
One common problem patients with heart failure face is fluid retention and swelling. If you notice new or worsening swelling, it may be useful to read about heart failure edema to understand causes and early management steps.
Conclusion
The fantastic four ARNI, betablocker, MRA, and SGLT2 inhibitor are more than just a list of pills. Theyre a proven, evidencebacked strategy that tackles heart failure from every angle: pressure, rhythm, fluid, and metabolism. By understanding both the benefits and the possible downsides, you can have a real, open conversation with your cardiologist and feel confident about the plan thats laid out for you.
Take the next step: download the free medicationchecklist, talk to your doctor about which of these drugs fit your health picture, and keep track of how you feel as you start each new dose. Remember, youre not alone in this journey the medical community, research studies, and countless patients walking the same path are all here to support you. Stay curious, stay proactive, and give your heart the best chance to keep beating strong.